
Abstract
Objective
To identify whether intraventricular hemorrhage (IVH) and cerebellar hemorrhage (CH) have common or divergent risk factors.
Study design
This is a retrospective cross-sectional cohort of infants including all infants born <30 weeks from 2007 to 2016. Comprehensive perinatal and clinical factors were extracted from the medical record. Outborn infants, infants with major congenital anomaly, those transferred prior to discharge, and those with mixed or no brain injury were excluded. The remaining infants were divided into two groups: IVH only and CH only. Continuous variables were evaluated with the Wilcoxon–Mann–Whitney test, and categorical variables were evaluated with Fisher’s exact test. Multinomial logistic regression was used to identify factors which predispose infants towards injury type more than another, holding other factors constant.
Results
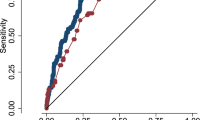
In total, 127 infants were included (CH n = 27, IVH n = 100). Compared to those with IVH, infants with CH were of lower EGA (p = 0.03), lower birth weight (p = 0.01), more often of multiple gestation (p = 0.03), more frequently born emergently (p = 0.03), had a greater number of ventilator days (p = 0.03), received postnatal steroids more often (p = 0.02), had a greater incidence of hemodynamically significant patent ductus arteriosus (PDA), and less frequently had pulmonary hemorrhage (p = 0.04). In multinomial regression analysis, three factors were identified which favored CH over IVH: multiple gestation (RR 4.70, 95% CI 1.56–14.21, p < 0.01), chorioamnionitis (RR 3.18, 95% CI 1.13–8.92, p = 0.03), and emergent delivery (RR 4.14, 95% CI 1.48–11.55, p < 0.01). Only advancing gestational favored IVH over CH (RR 0.74, 95% CI 0.65–0.85, p < 0.01).
Conclusions
IVH and CH have unique risk factors. These results highlight the need to tailor neuroimaging surveillance to specific patient risk factors.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Volpe JJ. Neurology of the newborn. 5th ed. Philadelphia: Saunders/Elsevier; 2008.
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010;126:443–56
Wilson-Costello D, Friedman H, Minich N, Fanaroff AA, Hack M. Improved survival rates with increased neurodevelopmental disability for extremely low birth weight infants in the 1990s. Pediatrics.2005;115:997–1003.
Jain NJ, Kruse LK, Demissie K, Khandelwal M. Impact of mode of delivery on neonatal complications: trends between 1997 and 2005. J Matern Fetal Neonatal Med. 2009;22:491–500.
Mukerji A, Shah V, Shah PS. Periventricular/intraventricular hemorrhage and neurodevelopmental outcomes: a meta-analysis. Pediatrics. 2015;136:1132–43.
Papile LA, Munsick-Bruno G, Schaefer A. Relationship of cerebral intraventricular hemorrhage and early childhood neurologic handicaps. J Pediatr. 1983;103:273–7.
Cramer BC, Jequier S, O’Gorman AM. Sonography of the neonatal craniocervical junction. AJR Am J Roentgenol. 1986;147:133–9.
Di Salvo DN. A new view of the neonatal brain: clinical utility of supplemental neurologic US imaging windows. Radiographics.. 2001;21:943–55.
Sehgal A, El-Naggar W, Glanc P, Asztalos E. Risk factors and ultrasonographic profile of posterior fossa haemorrhages in preterm infants. J Paediatr Child Health. 2009;45:215–8.
Limperopoulos C, Benson CB, Bassan H, Disalvo DN, Kinnamon DD, Moore M, et al. Cerebellar hemorrhage in the preterm infant: ultrasonographic findings and risk factors. Pediatrics.2005;116:717–24.
Limperopoulos C, Bassan H, Gauvreau K, Robertson RL, Sullivan NR, Benson CB, et al. Does cerebellar injury in premature infants contribute to the high prevalence of long-term cognitive, learning, and behavioral disability in survivors? Pediatrics. 2007;120:584–93.
Soul JS, Hammer PE, Tsuji M, Saul JP, Bassan H, Limperopoulos C, et al. Fluctuating pressure-passivity is common in the cerebral circulation of sick premature infants. Pediatr Res. 2007;61:467–73.
Vesoulis ZA, Ters NE, Foster A, Trivedi SB, Liao SM, Mathur AM, Response to dopamine in prematurity: a biomarker for brain injury?. J Perinatol J Calif Perinat Assoc.. 2016;36:453–8.
Osborn DA, Evans N, Kluckow M. Hemodynamic and antecedent risk factors of early and late periventricular/intraventricular hemorrhage in premature infants. Pediatrics. 2003;112:33–9.
Noori S, McCoy M, Anderson MP, Ramji F, Seri I, Changes in cardiac function and cerebral blood flow in relation to peri/intraventricular hemorrhage in extremely preterm infants. J Pediatr. 2014;164:264–70.e3
Sellmer A, Bjerre JV, Schmidt MR, McNamara PJ, Hjortdal VE, Høst B, et al Morbidity and mortality in preterm neonates with patent ductus arteriosus on day 3. Arch Dis Child Fetal Neonatal Ed.2013;98:F505–10.
Liebowitz M, Clyman RI. Antenatal betamethasone: a prolonged time interval from administration to delivery is associated with an increased incidence of severe intraventricular hemorrhage in infants born before 28 weeks gestation. J Pediatr.2016;177:114–20.e1.
Ment LR, Oh W, Ehrenkranz RA, Philip AG, Duncan CC, Makuch RW. Antenatal steroids, delivery mode, and intraventricular hemorrhage in preterm infants. Am J Obstet Gynecol. 1995;172:795–800.
Gano D, Ho M-L, Partridge JC, Glass HC, Xu D, Barkovich AJ, et al. Antenatal exposure to magnesium sulfate is associated with reduced cerebellar hemorrhage in preterm newborns. J Pediatr. 2016;178:68–74.
Crowther CA, Hiller JE, Doyle LW, Haslam RR, Australasian Collaborative Trial of Magnesium Sulphate (ACTOMg SO4) Collaborative Group. Effect of magnesium sulfate given for neuroprotection before preterm birth: a randomized controlled trial. JAMA. 2003;290:2669–76.
Marret S, Marpeau L, Zupan-Simunek V, Eurin D, Lévêque C, Hellot M-F, et al. Magnesium sulphate given before very-preterm birth to protect infant brain: the randomised controlled PREMAG trial*. BJOG Int J Obstet Gynaecol. 2007;114:310–8.
Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM, et al. A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. N Engl J Med. 2008;359:895–905.
Sugimoto J, Romani AM, Valentin-Torres AM, Luciano AA, Ramirez Kitchen CM, Funderburg N, et al. Magnesium decreases inflammatory cytokine production: a novel innate immunomodulatory mechanism. J Immunol. 2012;188:6338–46.
Levene MI, Fawer CL, Lamont RF. Risk factors in the development of intraventricular haemorrhage in the preterm neonate. Arch Dis Child.1982;57:410.
Miller SS, Lee HC, Gould JB. Hypothermia in very low birth weight infants: distribution, risk factors and outcomes. J Perinatol. 2011;31:S49–56.
Bissinger RL, Annibale DJ. Thermoregulation in very low-birth-weight infants during the golden hour: results and implications. Adv Neonatal Care. 2010;10:230–8.
Reynolds RD, Pilcher J, Ring A, Johnson R, McKinley P. The golden hour: care of the LBW infant during the first hour of life one unit’s experience. Neonatal Netw J Neonatal Nurs.2009;28:211–9.
Lyu Y, Shah PS, Ye XY, Warre R, Piedboeuf B, Deshpandey A, et al. Association between admission temperature and mortality and major morbidity in preterm infants born at fewer than 33 weeks’ gestation. JAMA Pediatr.2015;169:e150277.
Laptook AR, Salhab W, Bhaskar B, Neonatal Research Network. Admission temperature of low birth weight infants: predictors and associated morbidities. Pediatrics. 2007;119:e643–9.
Acknowledgements
The authors wish to acknowledge the assistance of Amy Distler, RN in the identification of infants with cerebellar hemorrhage.
Funding
This work was supported by the following grants: 1. Washington University Institute of Clinical and Translational Sciences KL2 Training Program (NIH/NCATS KL2 TR000450). 2. The Barnes-Jewish Hospital Foundation and the Washington University Institute of Clinical and Translational Sciences Clinical and Translational Funding Program (NIH/NCATS UL1 TR000448). 3. Washington University in St. Louis Center for Biomedical Informatics, Clinical Investigation Data Exploration Repository (NIH/NCATS UL1 TR000448).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Vesoulis, Z.A., Herco, M. & Mathur, A.M. Divergent risk factors for cerebellar and intraventricular hemorrhage. J Perinatol 38, 278–284 (2018). https://doi.org/10.1038/s41372-017-0010-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-017-0010-x
