
Abstract
The paucity of information on longevity of vaccine-induced immune responses and uncertainty of the correlates of protection hinder the development of evidence-based COVID-19 vaccination policies for new birth cohorts. Here, to address these knowledge gaps, we conducted a cohort study of healthy 5–12-year-olds vaccinated with BNT162b2. We serially measured binding and neutralizing antibody titers (nAbs), spike-specific memory B cell (MBC) and spike-reactive T cell responses over 1 year. We found that children mounted antibody, MBC and T cell responses after two doses of BNT162b2, with higher antibody and T cell responses than adults 6 months after vaccination. A booster (third) dose only improved antibody titers without impacting MBC and T cell responses. Among children with hybrid immunity, nAbs and T cell responses were highest in those infected after two vaccine doses. Binding IgG titers, MBC and T cell responses were predictive, with T cells being the most important predictor of protection against symptomatic infection before hybrid immunity; nAbs only correlated with protection after hybrid immunity. The stable MBC and T cell responses over time suggest sustained protection against symptomatic SARS-CoV-2 infection, even when nAbs wane. Booster vaccinations do not confer additional immunological protection to healthy children.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout






Similar content being viewed by others


Data availability
All aggregate data supporting the findings of this study are available within the paper and its supplementary materials. Individual-level participant data are not publicly available. Only the data of individuals who consented to further research can be accessible with the consent of the ethics committees from the requestor’s and corresponding authors’ institutions. A formal data transfer agreement between the institutions will be required upon ethics approval. The corresponding authors can be contacted for access to data and will respond within 1 month; data transfer can take place once the data transfer agreement is completed.
References
World Health Organization. Interim statement on hybrid immunity and increasing population seroprevalence rates. https://www.who.int/news/item/01-06-2022-interim-statement-on-hybrid-immunity-and-increasing-population-seroprevalence-rates (2022).
Goldblatt, D., Alter, G., Crotty, S. & Plotkin, S. A. Correlates of protection against SARS-CoV-2 infection and COVID-19 disease. Immunol. Rev. 310, 6–26 (2022).
Khoury, D. S. et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 27, 1205–1211 (2021).
Wherry, E. J. & Barouch, D. H. T cell immunity to COVID-19 vaccines. Science 377, 821–822 (2022).
Bertoletti, A., Le Bert, N. & Tan, A. T. SARS-CoV-2-specific T cells in the changing landscape of the COVID-19 pandemic. Immunity 55, 1764–1778 (2022).
Kent, S. J. et al. Disentangling the relative importance of T cell responses in COVID-19: leading actors or supporting cast? Nat. Rev. Immunol. 22, 387–397 (2022).
Kalimuddin, S. et al. Early T cell and binding antibody responses are associated with COVID-19 RNA vaccine efficacy onset. Medicine 2, 682–688 (2021).
Tan, A. T. et al. Rapid measurement of SARS-CoV-2 spike T cells in whole blood from vaccinated and naturally infected individuals. J. Clin. Investig. 131, e152379 (2021).
Samandari, T. et al. Prevalence and functional profile of SARS-CoV-2 T cells in asymptomatic Kenyan adults. J. Clin. Investig. 133, e170011 (2023).
Le Bert, N. et al. Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection. J. Exp. Med. 218, e20202617 (2021).
Ogbe, A. et al. T cell assays differentiate clinical and subclinical SARS-CoV-2 infections from cross-reactive antiviral responses. Nat. Commun. 12, 2055 (2021).
Sette, A. & Crotty, S. Immunological memory to SARS-CoV-2 infection and COVID-19 vaccines. Immunol. Rev. 310, 27–46 (2022).
Andreano, E. et al. Hybrid immunity improves B cells and antibodies against SARS-CoV-2 variants. Nature 600, 530–535 (2021).
Suryawanshi, R. & Ott, M. SARS-CoV-2 hybrid immunity: silver bullet or silver lining? Nat. Rev. Immunol. 22, 591–592 (2022).
Centers for Disease Control and Prevention. COVID-19 vaccine: interim COVID-19 immunization schedule for persons 6 months of age and older. https://broadwaymedicalclinic.com/wp-content/uploads/2020/04/covid-19-immunization-schedule-ages-6months-older.pdf (2023).
Royal College of Paediatrics and Child Health. RCPCH statement in response to JCVI advice on offering COVID-19 vaccination to all 5–11-year-olds. https://www.rcpch.ac.uk/news-events/news/rcpch-statement-response-jcvi-advice-offering-covid-19-vaccination-all-5-11-year (2022).
European Medicines Agency. Comirnaty. https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (2021).
Ministry of Health Singapore. Child vaccination. https://www.moh.gov.sg/covid-19/vaccination/child (2021).
Feng, S. et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 27, 2032–2040 (2021).
Corbett, K. S. et al. Immune correlates of protection by mRNA-1273 vaccine against SARS-CoV-2 in nonhuman primates. Science 373, eabj0299 (2021).
Earle, K. A. et al. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 39, 4423–4428 (2021).
Khoury, D. S. et al. Predicting the efficacy of variant-modified COVID-19 vaccine boosters. Nat. Med. 29, 574–578 (2023).
Cromer, D. et al. Neutralising antibody titres as predictors of protection against SARS-COV-2 variants and the impact of boosting: a meta-analysis. Lancet Microbe https://doi.org/10.1016/s2666-5247(21)00267-6 (2022).
Gilbert, P. B. et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 375, 43–50 (2022).
Dowell, A. C. et al. Association of spike-specific T cells with relative protection from subsequent SARS-CoV-2 Omicron infection in young children. JAMA Pediatr. 177, 96–97 (2023).
Tan, A. T. et al. Early induction of functional SARS-CoV-2-specific T cells associates with rapid viral clearance and mild disease in COVID-19 patients. Cell Rep. 34, 108728 (2021).
Rydyznski Moderbacher, C. et al. Antigen-specific adaptive immunity to SARS-CoV-2 in acute COVID-19 and associations with age and disease severity. Cell 183, 996–1012 (2020).
Bertoletti, A. et al. SARS-CoV-2-specific T cells in infection and vaccination. Cell Mol. Immunol. 18, 2307–2312 (2021).
Carabelli, A. M. et al. SARS-CoV-2 variant biology: immune escape, transmission and fitness. Nat. Rev. Microbiol. 21, 162–177 (2023).
Painter, M. M. et al. Prior vaccination promotes early activation of memory T cells and enhances immune responses during SARS-CoV-2 breakthrough infection. Nat. Immunol. 24, 1711–1724 (2023).
Crotty, S. Hybrid immunity. Science 372, 1392–1393 (2021).
Goel, R. R. et al. Distinct antibody and memory B cell responses in SARS-CoV-2 naïve and recovered individuals following mRNA vaccination. Sci. Immunol. 6, eabi6950 (2021).
Goel, R. R. et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 374, abm0829 (2021).
Yung, C. F. et al. BNT162b2 vaccine protection against omicron and effect of previous infection variant and vaccination sequence among children and adolescents in Singapore: a population-based cohort study. Lancet Child Adolesc. Health 7, 463–470 (2023).
Plotkin, S. A. Correlates of protection induced by vaccination. Clin. Vaccin. Immunol. 17, 1055–1065 (2010).
Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 23, 186–193 (2022).
McMahan, K. et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature 590, 630–634 (2021).
Madelon, N. et al. Robust T-cell responses in anti-CD20-treated patients following COVID-19 vaccination: a prospective cohort study. Clin. Infect. Dis. 75, e1037–e1045 (2022).
Md Yusof, M. Y. et al. Breakthrough SARS-CoV-2 infections and prediction of moderate-to-severe outcomes during rituximab therapy in patients with rheumatic and musculoskeletal diseases in the UK: a single-centre cohort study. Lancet Rheumatol. 5, e88–e98 (2023).
Cho, A. et al. Anti-SARS-CoV-2 receptor-binding domain antibody evolution after mRNA vaccination. Nature 600, 517–522 (2021).
Mateus, J. et al. Low-dose mRNA-1273 COVID-19 vaccine generates durable memory enhanced by cross-reactive T cells. Science 374, eabj9853 (2021).
Chia, W. N. et al. Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: a longitudinal study. Lancet Microbe 2, e240–e249 (2021).
Tulsian, N. K. et al. Defining neutralization and allostery by antibodies against COVID-19 variants. Nat. Commun. https://doi.org/10.1038/s41467-023-42408-x (2023).
Tan, C. W. et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 38, 1073–1078 (2020).
Tan, C. W. et al. Pan-sarbecovirus neutralizing antibodies in BNT162b2-immunized SARS-CoV-1 survivors. N. Engl. J. Med. 385, 1401–1406 (2021).
Tan, C. W. et al. Comparative neutralisation profile of SARS-CoV-2 Omicron subvariants BA.2.75 and BA.5. Lancet Microbe 3, e898 (2022).
Gaebler, C. et al. Evolution of antibody immunity to SARS-CoV-2. Nature 591, 639–644 (2021).
Sokal, A. et al. Maturation and persistence of the anti-SARS-CoV-2 memory B cell response. Cell 184, 1201–1213 (2021).
Wang, Z. et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature 592, 616–622 (2021).
Acknowledgements
We gratefully acknowledge the support from A. Bertoletti and A. Tanoto Tan for suggestions on data interpretation; E. Shuyi Gan, T. Siriphanitchakorn, Y. S. Leong, K. W. Teng, C. Qui and M. Qui from Duke-NUS and C.-H. Huang, G. C. Yap, H. Wen, B. Shunmuganathan and R. Gupta from NUS for technical assistance; clinical research coordinators S. Wong, J. Lim, J. Yap, R. Chua and N. Siti Binte Roslan from NUH for assistance with participant recruitment and follow-up; and S. Nishanti Ramasamy for assistance with manuscript editing, formatting and submission. E.H.T. is supported by the National Medical Research Council (NMRC) Transition Award (MOH-000269), C.W.T. is supported by the NMRC Open Fund – Large Collaborative Grant (OFLCG19May-0034) and the National University of Singapore Startup grant (NUHSRO/2023/018/Startup/10) and E.E.O. is supported by the NMRC Singapore Translational Research (STaR) Award (MOH-001271-00). This study was supported by the NUS award of E.H.T. (NUHSRO/2021/081/NUS Med/07/MARVELS) from the Yong Loo Lin School of Medicine. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. Most of all, we gratefully acknowledge the heroic efforts of all the children and families who gave their precious time and biosamples to the MARVELS study.
Author information
Authors and Affiliations
Contributions
Y.Z., L.P.S., E.H.T. and E.E.O. designed and conceptualized the pediatric MARVELS study. J.G.L. designed and conceptualized the adult healthcare worker study used for comparison. L.P.S. and E.H.T. acquired funding and supervised the project. A.Y.H.K., C.J.X.T., H.E.L., N.E., W.C.Y., C.W.T., J.M.E.L. and N.L.B. provided administrative, technical and material support. Y.Z. and C.J.X.T. performed the statistical analyses. Y.Z., K.R.C., E.Z.O. and E.E.O. interpreted the data. Y.Z. and E.E.O. wrote the paper. All authors contributed to the revision of the paper and approved the final version for publication.
Corresponding authors
Ethics declarations
Competing interests
N.L.B. reports a patent for a method to monitor SARS-CoV-2-specific T cells in biological samples, which is pending. The other authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks the anonymous reviewers for their contribution to the peer review of this work. Primary Handling Editor: Alison Farrell, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
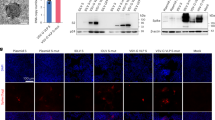
Extended Data Fig. 1 Isotypes and binding activity of Spike-specific memory B cells (S + MBC) in children with immunity against SARS-CoV-2.
A. Representative flow cytometric staining plots for vaccine-only (VV), hybrid (VVI), and infection-only immunity (n = 1 each). B. S + MBC isotypes in children with vaccine-only immunity (n = 34), at pre-vaccination baseline, and 3- and 6 months post vaccination. C. Binding activity against Spike proteins from three SARS-CoV-2 variants in B cell ELISPOT. Spike-specific memory B cells (S+ MBCs) were extracted from a pediatric subject 3 months after 2 doses of mRNA BNT162b2, and then cultured and differentiated ex vivo into antibody secreting cells.
Extended Data Fig. 2 Children vaccinated with 2 doses of mRNA SARS-CoV-2 vaccine have low levels of Th2 cytokines (n = 34).
A, B, C. Spike-reactive Th2 responses, measured by interleukin-4, interleukin-5 and interleukin-13 for children with vaccine-only immunity, and adults. For box-whisker graphs, upper and lower boundaries of boxes indicate upper and lower quartile respectively, line indicates median, and whiskers represent the range.
Extended Data Fig. 3 Vaccine-associated local and systemic adverse events and symptoms of SARS-CoV-2 infection reported by MARVELS children.
A. Percentages and severity of parent and / or subject – reported local and systemic symptoms for 10 days after vaccination. Blue = adverse events after doses 1 and 2, with color gradient representing spectrum of severity; Red = adverse events after booster (dose 3), with color gradient representing spectrum of severity. B. Clinical features of symptomatic SARS-CoV-2 infections for all episodes of symptomatic SARS-CoV-2 infection among vaccinated children. Two-tailed Fisher’s exact test was used for comparison between groups; ns: not significant, *: p ≤ 0.05, **: p ≤ 0.01, ***: p ≤ 0.001, ****: p ≤ 0.0001. For pain at injection site, p-value = 0.0189. For fever, p-value = 0.0091.
Extended Data Fig. 4 Nucleocapsid (N)-specific antibodies and T cells in children with asymptomatic SARS-CoV-2 infections.
A. Venn diagram showing all episodes of asymptomatic COVID-19 identified in this study (n = 30), separated into whether they were identified via seropositivity, T cell reactivity, or both against SARS-CoV-2 N protein. B, C. N-reactive T cell responses measured by post-stimulation interferon-γ and interleukin-2 levels, at pre-vaccination baseline, 3- and 6 months post vaccination, from vaccinated (two doses) children who remained uninfected (VV, n = 34), with symptomatic infection (VVI(S), n = 49) and asymptomatic infection (VVI(A), n = 11). D. N-reactive T cell responses measured by post-stimulation interferon-γ and E. interleukin-2 levels, at 6- and 12 months post vaccination, for VV children at 6 months. F. N-reactive T cell responses measured by post-stimulation interferon-γ and G. interleukin-2 levels, at 6- and 12 months post vaccination, for children with hybrid immunity at 6 months. In D-G, children were grouped into the following categories: 1) Those who did not develop SARS-CoV-2 infection between 6 and 12 months, 2) those who developed symptomatic SARS-CoV-2 re-infection (S), or 3) those who had asymptomatic re-infection. In all graphs, subjects with serological evidence of asymptomatic SARS-CoV-2 are colored in blue.
Extended Data Fig. 5 The proximity of last immunity-boosting event is similar for children who had symptomatic SARS-CoV-2 infection between doses 1 and 2 (VIV), and children who had symptomatic SARS-CoV-2 infection after 2 doses (VVI(S)).
A. Schematic representation of the different last immunity-boosting event, for VIV and VVI(S) children. Created with BioRender.com. B. Comparison of proximity of immunity-boosting event for VIV and VVI(S) children. For box-whisker graphs, upper and lower boundaries of boxes indicate upper and lower quartile respectively, line indicates median, and whiskers represent the range. Two-tailed Mann–Whitney U test was used for comparison between groups; ns: not significant, *: p ≤ 0.05, **: p ≤ 0.01, ***: p ≤ 0.001, ****: p ≤ 0.0001.
Extended Data Fig. 6 Eight-cytokines measured in the cytokine release assay for Spike-reactive T cell responses among children with hybrid immunity.
A. Schematic of cytokine release assay and analytical methods (after DMSO control subtraction) using unsupervised clustering algorithm (UMAP). The cytokines quantified were interferon-γ (IFN-γ), interleukin-2 (IL-2), tumor necrosis factor-α (TNF-α), Granzyme-B, interleukin-10 (IL-10), interleukin-4 (IL-4), interleukin-5 (IL-5), and interleukin-13 (IL-13). B. UMAP plots generated with all analyzed samples (n = 391, consisting of adults, infected children and vaccinated children at all time points) with levels of secreted cytokines shown in heatmaps. C. Concatenated cytokine secretion profiles of S peptide pool-stimulated whole blood from children with VIV, VVI(S) and VVI(A). Cytokine secretion profiles were overlaid on the global UMAP plot of all analyzed samples (black dots; each dot corresponds to one culture supernatant).
Extended Data Fig. 7 Immune correlates of protection against symptomatic SARS-CoV-2 infection between 3- and 6 months from start of vaccination.
N = 23 children had symptomatic SARS-CoV-2 infection between months 3 and 6, while n = 66 did not; of these, n = 3 had asymptomatic SARS-CoV-2 infection. A. 3-month Spike (S)-reactive T cell responses, quantified using interferon- γ (IFN-γ) and interleukin-2 (IL-2), for children with no infection, symptomatic and asymptomatic SARS-CoV-2 infection between 3 and 6 months. For comparison between no infection and symptomatic infection, p-value for IFN-γ = 0.000688 and for IL-2 = 0.025786. For comparison between symptomatic infection and asymptomatic infection, p-value for IFN-γ = 0.015810 and for IL-2 = 0.031621. B. 3-month Omicron BA.2 pVNT50 titers in children who did and did not develop symptomatic SARS-CoV-2 infection between 3 and 6 months. Color of dots indicate the type of pre-existing immunity they had at month 3 (p-value = 0.000589). C. Receiver operator characteristics (ROC) curve for BA.2 measured at 3 months from start of vaccination. D. pVNT50 titers Anti-S IgG titers, E. Percentage of S+ MBCs out of total B cells (p-value 0.004599), and F. S-reactive T cell responses measured by post-stimulation interferon-γ levels at month 3 post-vaccination (p-value 0.047200), for VVI(S) and non-VVI(S) children with and without symptomatic SARS-CoV-2 infection. For box-whisker graphs, upper and lower boundaries of boxes indicate upper and lower quartile respectively, line indicates median, and whiskers represent the range. Two-tailed Mann–Whitney U test was used to compare between groups. The ROC curve analysis was performed using the Wilson/Brown test. ns: not significant, *: p ≤ 0.05, **: p ≤ 0.01, ***: p ≤ 0.001, ****: p ≤ 0.0001.
Extended Data Fig. 8 Protection from symptomatic SARS-CoV-2 infection was associated with hybrid immunity but not age.
A. Superior protective capacity of hybrid immunity, demonstrated by the different in percentages of children who developed symptomatic SARS-CoV-2 infection between 6 and 12 months, among children with vaccine-only (VV) immunity at 6 months, compared to children with hybrid immunity at 6 months. Two-tailed Fisher’s exact test was used for comparison between groups. P-value = 0.0018. B, C. Symptomatic SARS-CoV-2 infection was not associated with age, as demonstrated by B. age distribution of all children getting their first infection after 2 doses of mRNA vaccination (n = 57 symptomatic, n = 16 asymptomatic), and C. age distribution of all children with hybrid immunity getting a re-infection (n = 3 symptomatic and n = 11 asymptomatic). For box-whisker graphs, upper and lower boundaries of boxes indicate upper and lower quartile respectively, line indicates median, and whiskers represent the range. Two-tailed Mann–Whitney U test was used to compare between different groups. ns: not significant, *: p ≤ 0.05, **: p ≤ 0.01, ***: p ≤ 0.001, ****: p ≤ 0.0001.
Supplementary information
Supplementary Information
Supplementary Fig. 1 and Table 1.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhong, Y., Kang, A.Y.H., Tay, C.J.X. et al. Correlates of protection against symptomatic SARS-CoV-2 in vaccinated children. Nat Med (2024). https://doi.org/10.1038/s41591-024-02962-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41591-024-02962-3
