
Abstract
Aims
To evaluate the safety and efficacy of propofol sedation combined with sub-Tenon's anaesthesia for strabismus surgery in adults.
Methods
Thirty-two consecutive patients aged 31–85 years underwent strabismus surgery under general (n=16) or local (n=16) anaesthesia. In the local anaesthesia (study) group, sedation was induced with a loading dose of midazolam, fentanyl, and propofol, followed by continuous infusion of propofol, 3–6 mg/k/h to deep sedation. A nasal tube was inserted to prevent airway obstruction. Sub-Tenon's anaesthesia included infusion of a 3–4 ml mixture (50 : 50) of lidocaine 2%/mercaine 0.5%. General anaesthesia consisted of premedication with midazolam, followed by fentanyl, esmeron-bromate, propofol, and tracheal intubation. Duration of surgery and anaesthesia, intraoperative oculocardiac reflex and arrhythmias, time to discharge, postoperative pain, nausea and vomiting, and patient and surgeon satisfaction were evaluated.
Results
The local anaesthesia group had a significantly shorter operative and anaesthesia time, fewer episodes of oculocardiac reflex or arrythmia/bradycardia requiring treatment, fewer early or late episodes of nausea and vomiting, and less pain. The patients and surgeon in this group reported higher satisfaction.
Conclusion
Propofol sedation with local sub-Tenon's injection of lidocaine/mercaine is recommended for the induction and maintenance of anaesthesia during unilateral or bilateral strabismus surgery in adults. The method is quick and effective, without systemic or ocular side effects.
Similar content being viewed by others

Introduction
For proper anaesthesia during strabismus surgery, both the general condition of the patient and the akinesia of the extraocular muscles (EOMs) need to be monitored, with consideration of patient comfort and pain. Today, surgery may be performed with less morbidity compared to the past using general,1, 2, 3, 4 retrobulbar,5, 6, 7, 8, 9, 10, 11 or peribulbar anaesthesia,11, 12, 13, 14 sub-Tenon's anaesthesia,15, 16, 17, 18, 19, 20 or combinations of sedation/topical,21, 22 sedation/peribulbar,23 and sedation/local techniques.24 General anaesthesia,1, 2, 3, 4 however, involves more risk of serious cardiac, respiratory, and central nervous system complications. Retrobulbar6, 7, 8, 9, 11, 19 and peribulbar11, 13, 14, 25 anaesthesia may be associated with these same risks from inadvertent injection of the agents into the venous system or central nervous system, as well as with ocular complications, such as globe perforation, retrobulbar haemorrhage, retinal vascular occlusion, optic nerve injury, contralateral amaurosis, and general disorientation. Topical anaesthesia,21, 22, 26 alone or combined with sedation, may cause ocular pain or pressure. We hypothesized that propofol sedation combined with sub-Tenon's injection of lidocaine (Esracaine) 2% and mercaine 0.5% to the retrobulbar space would increase the anaesthetic efficacy and avoid the side effects of the other methods. It might also be feasible for use in high-risk adult patients with serious comorbidities.
Patients and methods
The study sample included 32 consecutive patients who underwent strabismus surgery at our major university-affiliated centre from 2001 to 2003. Inclusion criteria were age ⩾30 years (prompted by our previous experience), presence of horizontal or cyclovertical strabismus (excluding superior oblique procedures), and no previous EOM surgery, retinal detachment, or filter operation. Patients with ocular or neurological problems, mental retardation, deafness, or dementia were excluded. Institutional review board approval was not necessary because the operations were performed according to departmental policy at the time.
Complete preoperative physical, ophthalmologic, and orthoptic examinations were performed, and patients were classified according to the American Society of Anesthesiologists (ASA) score and New York Heart Association (NYHA) grade. From June 2001 to December 2002, general anaesthesia was used in all patients (control group, n=16), and from January 2003 to June 2004, sedation/local sub-Tenon's anaesthesia was used in all consecutive patients in the study (study group, n=16). The study patients received premedication with oral midazolam 5 mg and topical benoxinate HCl 0.4% (Localin, Fisher Laboratories, Israel), three drops every 5 min into the lower conjunctival cul-de-sac fornix, followed by two applications of Esracaine gel 2% (Rafa Laboratories, Jerusalem, Israel). During surgery, 30% oxygen at 3–5 l/min was administered via a double nasal cannula. For sedation, we used a loading dose of midazolam 0–1 mg (Rafa Laboratories), fentanyl 25–100 μg (Taro Pharmaceutical Industries Ltd, Haifa, Israel), and propofol 1–2 mg/g (Diprivan, B Braun, Melsungen, Germany), followed by continuous infusion of propofol 3–6 mg/k/h, titrated until the patient was deeply sedated but still breathing spontaneously; the dosages were adjusted according to the patient's age, health, and weight. A nasal airway tube was inserted immediately in 13/16 patients after deep sedation was achieved to prevent snore sign, jaw thrust, or paradoxical movements.
The general anaesthesia procedure included premedication with oral midazolam 5 mg, followed by intravenous induction with fentanyl 2 μg/kg, propofol (Diprivan) 2.5 mg/kg, and rocuronium bromide (Esmeron, NV Organon, Holland) 0.6 mg/kg, and endotracheal intubation. Maintenance was achieved with inhaled nitrous oxide 69%, oxygen 30%, and isoflurane 1%.
All operations were performed by same surgeon (MS) using the same technique. A limbal or fornix incision was made near the muscle to be operated on through the conjunctiva and Tenon's capsule, down to the bare sclera. A blunt, 19-Gauge irrigation cannula was advanced along the globe into the sub-Tenon's space for infusion of a 3–4 ml mixture (50 : 50) of lidocaine 2% (Esracaine-HCl 2%, Rafa Laboratories) and mercaine 0.5% (Bupivocaine, Beit-Kama, Israel). After waiting for 5 min for pupillary dilation, we proceeded to the planned EOM surgery (Table 1). Supplemental local anaesthesia was given as necessary.
All patients in both groups received 20 mg intravenous dexamethasone at the conclusion of surgery.
The hospital discharge decision in both groups was made by the attending anaesthesiologist on the basis of patient request, the Day Care Unit nurse evaluation, and the Aldrete postanaesthesia score.27
To evaluate the effectiveness and safety of combined propofol/sub-Tenon's anaesthesia in unilateral or bilateral strabismus surgery, the study and control groups were compared for nine parameters: (1) duration of surgery; (2) duration of anaesthesia from induction to recovery of alertness; (3) oculocardiac reflex (OCR), defined as an acute decrease in heart rate induced by pressure on the eye or traction of an EOM; (4) cardiac arrhythmia following surgery; (5) discharge time, calculated from the end of surgery to discharge from the hospital; 6) Visual Analog Scale (VAS) score (0–10) for postoperative pain, completed by the patient in the recovery room and at home during the first 24 h after surgery; (7) postoperative nausea and vomiting (PONV) episodes in the recovery room and at home in the first 24 h after surgery; (8) patient satisfaction with anaesthesia, scored on a scale of 0 (dissatisfaction) to 10 (maximal satisfaction); and (9) surgeon satisfaction, scored on a scale of 0–10.
Statistical analysis
χ2 test was performed to evaluate between-group differences in sex distribution, ASA/NYHA scores, arrhythmia and OCR, number of operated EOMs, postoperative PONV in hospital and 24 h after surgery, and patient and surgeon satisfaction. Student's t-test was used to evaluate between-group differences in age, duration of anaesthesia and surgery, time from conclusion of surgery to discharge, and VAS score in hospital and 24 h postoperatively. In both groups, we analysed the correlation between the various main parameters and their impact using Pearson analysis. Life-table comparison was employed to compare differences in discharge time between groups.
A P-value of 0.05 or less was considered significant. The SPSS program (version 11.5/2003, Chicago, IL, USA) was used for all statistical calculations.
Results
The baseline data are shown in Table 1, and the operated EOMs in Table 2. Significant between-group differences were found for mean age (higher in the study group) and mean duration of surgery and anaesthesia and time to discharge (shorter in the study group) (Figures 1 and 2). Life-table analysis (Figure 2) showed that at 3 h after completion of surgery, 65% of the study group had been discharged compared to only 20% of the controls; corresponding rates at 4 h were 100 and 21%.

Duration of anaesthesia and surgery and time to discharge (in minutes) in the local and general anaesthesia groups.

Distribution (%) of discharge time (in min) in the local and general anaesthesia groups.
ASA and NYHA scores differed significantly between the groups. ASA II–III and NYHA II–III were found in 75 and 37.8%, respectively, of the sedation/local anaesthesia group and only 18.8% and none, respectively, of the control group (P=0.003, P=0.025, respectively), indicating a higher anaesthetic risk in the study group.
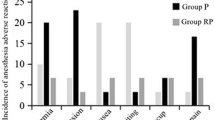
Intraoperatively, paradoxical movements occurred in three patients and were managed by nasal airway tubes. Thereafter, nasal tubes were inserted in another 13 patients prophylactically. Two patients required supplemental anaesthesia. Intraoperative cardiac arrhythmias occurred in one patient in each group, and they were sporadic and required no treatment. OCR occurred in three study patients (18.8%) and eight controls (50%) (P=0.06). Two study patients had short episodes of bradycardia (heart rate <40/min) at the beginning of the procedure, which disappeared without treatment, and four control patients (50%) had bradycardia, which required treatment with intravenous atropine.
The study group had significantly fewer PONV events immediately and 24 h after surgery (Table 1 and Figure 3). Four of the eight affected control patients (50%) required antiemetic treatment, immediately after surgery. In both groups, patients who vomited in hospital continued to do so at home. There was no correlation of duration of anaesthesia with nausea/vomiting.

Postoperative nausea/vomiting in the recovery room and at home (first 24 h) in the local and general anaesthesia groups.
Mean VAS score was significantly lower in the study group (Table 1 and Figure 4), both after surgery and 24 h later. Analgesia was required by 10 control patients (62.5%) immediately after surgery and by nine control patients (56.2%), 24 h later.

Mean VAS score in recovery room and at home (first 24 h) in the local and general anaesthesia groups.
Mean patient and surgeon satisfaction scores in hospital were higher in the study than the control group (Table 1 and Figure 5).

Mean satisfaction score of patients and surgeon.
Pearson correlation analysis showed that the patients in the study group who had a high VAS score in hospital also had a high score at home. In addition, the longer the duration of anaesthesia, the longer the time to discharge, which lowered patient satisfaction. There was a good correlation between patient and surgeon satisfaction, which increased as the duration of surgery and anaesthesia decreased.
Discussion
General anaesthesia is considered the gold standard in strabismus surgery for patients without severe general morbidity. This study shows that in adults, the combination of propofol sedation with local sub-Tenon's infusion of lidocaine 2%/mercaine 0.5% is associated with decreased operative and recovery time as well as a reduction in systemic complications. However, precautionary steps should be taken during induction, intubation, and extubation.
The analgesic effect of sub-Tenon's anaesthesia is apparently due to the blockage of the ciliary ganglia and short posterior nerves to the EOM. Technically, it has the advantage of eliminating the passage of a sharp needle behind the globe, thereby avoiding the risk of direct ocular damage. However, direct myotoxicity of the anaesthetic agents is still a problem. Niemi-Murola et al28 and Stevens and Restori29 found that with sub-Tenon's injection, the liquid accumulated in the anterior part of the orbit and later diffused into the back part of the orbital facial sheath of the eyeball, with good continuity between the posterior Tenon's capsule and the retrobulbar and muscle cone space. Ripat et al12, 13, 30 found sub-Tenon's anaesthesia to be precise and long-lasting, even when small volumes were used.
Our method has several unique aspects. Greenberg and Pollard24 used preoperative topical ocular tetracaine 0.5% drops and an intravenous bolus of fentanyl (1–1.5 μg/kg) followed by continuous infusion of intravenous propofol (25–75 μg/kg/min), titrated until deep sedation. Local anaesthesia consisted of irrigation with 1.0 ml lidocaine 2% and epinephrine under the belly of each muscle to be operated. By contrast, we included intensive preoperative topical ocular treatment and supplementary infusion of the sedative agent following onset of surgery. In addition, we inserted a nasal tube to prevent partial airway obstruction, agitation, and/or paradoxical movements during surgery. Finally, the anaesthetic mixture of lidocaine 2%/mercaine 0.5% was not placed under the belly of the operated muscles and did not involve ballooning of the conjunctiva–Tenon's space around the EOM.
Regarding propofol sedation, Wards et al31 found it to be associated with considerably faster emergence from anaesthesia and lesser time to extubation than general inhalation anaesthesia. This was true in our study as well. We attributed the significantly lower mean anaesthesia time in the study group directly to the sedation technique, rather than to the surgical technique, which remained the same throughout the study period. Similar findings were reported by others for propofol alone or combined with N2O or fentanyl and midazolam, thiopentone/halothane, and thiolenthal/halothane.1, 2, 3, 4, 32, 33 Although some authors found that propofol (owing to its parasympathetic effects) was associated with more OCR and atrioventricular rhythm disorders than other agents, such as sevoflurane,3, 34 halothane, or ketamine/midazolam,3 and a greater need for atropine treatment,3 in our series, OCR occurred less often in the study than the control group (19 vs 50%), as did bradycardia regarding treatment (0 vs 25%). Hence, the operative time was shorter in the study group because of fewer interruptions. These findings are noteworthy considering the higher anaesthetic risk (ASA) in the study group.
In our hospital, adults are kept for a few hours' observation after strabismus surgery, until vital signs are stable. Our local anaesthesia group had a significantly shorter discharge time than the control group: at 4 h (240 min), 100% had been discharged compared to 20% of the controls (life-table analysis). These findings agree with the study of Greenberg and Pollard24 wherein discharge rates at 150 min after surgery were 100% in the study group and 90% in the control group. Thus, the recovery time after general anaesthesia appears to be less predictable than that after sedation/local anaesthesia, which makes discharge time planning more difficult.
Propofol has known antiemetic properties, and patients awaken from anaesthesia without confusion or headache.35, 36 In our study, PONV episodes in hospital and during the first 24 h were significantly reduced in the study group, but were not correlated with anaesthesia time. This finding was supported by Gürkan et al3 in a study of children given propofol/N2O or sevoflurane anaesthesia (P<0.005 and P<0.05, respectively), and by Reimer et al37 in patients given propofol or thiopentone/halothane.
Postoperative pain differed significantly between the groups, and the majority of the control group needed analgesic treatment in hospital and at home. In the series of Steele et al,19 half the patients reported mild (42%) to moderate (8%) pain following EOM traction, and Boscia et al21 noted that their patients reported (mild) pain only during bipolar cauterization and conjunctival closure.
The relatively low rates of PONV and pain in our sub-Tenon's anaesthesia group and their more rapid recovery probably accounted for their higher satisfaction compared to controls. The physician, too, was more satisfied with the local anaesthesia technique, which avoided anaesthesia-related operating difficulties and adverse intraoperative patient reactions. None of the patients scheduled for local anaesthesia had to be switched to general anaesthesia. We speculate that the deep sedation level allowed the clinician better control of patient well-being and haemodynamic stability. Boscia et al21 reported slight operative (surgeon) difficulty in 66 of their 67 cases and moderate difficulty in one case.
General side effects of propofol include hypotension, respiratory depression, apnea, and risk of aspiration. Our use of a nasal tube prevented the airway obstruction and patient agitation during surgery that may be caused by respiratory depression or apnea. Several authors38, 39, 40, 41 reported retinal and ophthalmic artery occlusion after sub-Tenon's anaesthesia, presumably due to an elevation in ocular and orbital pressure above the mean ophthalmic artery or central retinal artery pressure. This complication may be transient38, 39 or associated with other complications, such as vertical diplopia (consistent with restriction of the inferior rectus muscles),40 in addition to orbital haemorrhage, orbital cellulitis, and central nervous system depression,41 Feibel and Guyton38 suggested other possible mechanisms of retinal damage by sub-Tenon's block, such as pressure on the central retinal artery or posterior ciliary arteries, or ocular vasoconstriction, leading to a decrease in ocular blood flow and a consequent reduction in ocular pulse amplitude and pulsatile blood flow. However, none of our patients sustained serious ocular injury, except for an edematous reaction of the Tenon's capsule and conjunctiva in the injected area. This may be attributable to our precautionary steps, namely, injecting no more than 3–4 ml of the mixture, not too posteriorly and not forcibly.
In conclusion, we recommend the use of local sub-Tenon's injection of lidocaine-mercaine with propofol sedation for induction and maintenance of anaesthesia during primary unilateral or bilateral strabismus surgery in adults, including patients with a high anaesthetic risk.
References
Vuyk J, Hennis PJ, Burm AG, de Voogt JW, Spierdijk J . Comparison of midazolam and propofol in combination with alfentanil for total intravenous anesthesia. Anesth Analg 1990; 71: 645–650.
Serin S, Elibol O, Susngurtekin H, Gonullu M . Comparison of halothane/thiopental and propofol anesthesia for strabismus surgery. Ophthalmologica 1999; 213: 224–227.
Gürkan Y, Kilickan L, Toker K . Propofol–nitrous oxide versus sevoflurane–nitrous oxide for strabismus surgery in children. Paediatr Anaesth 1999; 9: 495–499.
Snellen FT, Vanacker B, Aken HV . Propofol–nitrous oxide versus thiopental sodium-isoflurane–nitrous oxide for strabismus surgery in children. Can J Anaesth 1993; 5: 37–41.
Szmyd SM, Nelson LB, Calhoun JH, Harley RD . Retrobulbar anesthesia in strabismus surgery. Arch Ophthalmol 1984; 102: 1325–1327.
Ramsay RC, Knobloch WH . Ocular perforation following retrobulbar anesthesia for retinal detachment surgery. Am J Ophthalmol 1978; 88: 61–64.
Morgan CM, Schatz H, Vine AK, Cantrill HL, Davidorf FH, Gitter KA et al. Ocular complications associated with retrobulbar injections. Ophthalmology 1988; 95: 660–665.
Sullivan KL, Brown GC, Forman AR, Sergott RC, Flanagan JC . Retrobulbar anesthesia and retinal vascular obstruction. Ophthalmology 1983; 90: 373–377.
Paulter SE, Grizzard WS, Thompson LN, Wing GL . Blindness from retrobulbar injection into the optic nerve. Ophthalmic Surg 1986; 117: 334–337.
Friedberg HL, Kline Jr OR . Contralateral anaurosis after retrobulbar injection. Am J Ophthalmol 1986; 101: 688–690.
Duker JS, Belmont JB, Benson WE, Brooks Jr HL, Brown GC, Federman JL . Inadvertent globe perforation during retrobulbar and peribulbar anesthesia: patient characteristics, surgical management, and visual outcomes. Ophthalmology 1991; 98: 519–526.
Ripart J, Lefrant JY, de La Coussaye JE, Prat-Pradal D, Vivien B, Eledjam JJ . Peribulbar versus retrobulbar anesthesia for ophthalmic surgery: an anatomical comparison of extraconal and intraconal injections. Anesthesiology 2001; 94: 56–62.
Ripart J, Lefrant JY, Vivien B, Charavle P, Fabbro-Peray P, Jaussaud A . Ophthalmic regional anesthesia: medial canthus episcleral (sub-tenon) anesthesia is more efficient than peribulbar anesthesia. Anesthesiology 2000; 92: 1278–1285.
Wang HS . Peribulbar anesthesia for ophthalmic procedures. J Cataract Refract Surg 1988; 14: 441–443.
Capo H, Munoz M . Sub-tenon's lidocaine irrigation for strabismus surgery (letter). Ophthalmic Surg 1992; 23: 145.
Guise PA . Sub-Tenon anesthesia: a prospective study of 6000 blocks. Anesthesiology 2003; 98: 964–968.
Pianka P, Weintraub-Padova H, Lazar M, Geyer O . Effect of sub-Tenon's and peribulbar anesthesia on intraocular pressure and ocular pulse amplitude. J Cataract Refract Surg 2001; 27: 1221–1226.
Chang BYP, Hee WCL, Ling R, Broadway DC, Beigi B . Local anaesthetic techniques and pulsatile ocular blood flow. Br J Ophthalmol 2000; 84: 1260–1263.
Steele MA, Lavrich JB, Nelson LB, Koller HP . Sub-Tenon's infusion of local anesthetic for strabismus surgery. Ophthal Surg 1992; 23: 40–43.
Davis DB, Mandel MR . Posterior peribulbar anesthesia: an alternative to retrobulbar anesthesia. J Cataract Refract Surg 1986; 12: 182–184.
Boscia F, La Tegola MG, Columbo G, Alessio G, Sborgia C . Combined topical anesthesia and sedation for open-globe injuries in selected patients. Ophthalmology 2003; 110: 1555–1559.
Diamond GR . Topical anesthesia for strabismus surgery. J Pediatr Ophthalmol Strab 1989; 26: 86–90.
Habib NE, Balmer HG, Hocking G . Efficacy and safety of sedation with propofol in peribulbar anaesthesia. Eye 2002; 16: 60–62.
Greenberg MF, Pollard ZF . Adult strabismus surgery under propofol sedation with local versus general anesthesia. J Am Assoc Ped Ophthalmol Strabismus 2003; 7: 116–120.
Sanders RJ, Nelson LB, Deutsch JA . Peribulbar anesthesia for strabismus surgery. Am J Ophthalmol 1990; 109: 705–708.
Klepper ID, Sanders LD, Rosen M (eds) Ambulatory Anaesthesia and Sedation. Impairment and Recovery. chapter 17 Blackwell Scientific Publications: Oxford, 1991, p 197.
Jacobi PC, Dietlein TS, Jacobi FK . A comparative study of topical vs retrobulbar anesthesia in complicated cataract surgery. Arch Ophthalmol 2000; 118: 1037–1043.
Stevens JD, Restori M . Ultrasound imaging of no-needle 1-quadrant sub-Tenon local anaesthesia for cataract surgery. Eur J Implant Refract Surg 1993; 5: 35–38.
Niemi-Murola L, Krootila K, Kivisaari R, Kangasmäki A, Kivisaari L, Maunuksela EL . Localization of local anesthetic solution by magnetic resonance imaging. Ophthalmology 2004; 111: 342–347.
Ripart J, Metge L, Prat-Pradal D, Lopez FM, Eledjam JJ . Medial canthus single-injection episcleral (sub-tenon anesthesia): computed tomography imaging. Anesth Analg 1998; 87: 42–45.
Ward JB, Niffenegger AS, Lavin CW, Acquadro MA, Ahern DK, Smith PV . The use of propofol and mivacurium anesthetic technique for the immediate postoperative adjustment of sutures in strabismus surgery. Ophthalmology 1995; 102: 122–128.
Larsson S, Asgeirsson B, Magnusson J . Propofol fentanyl anesthesia compared to thiopental-halothane with special reference to recovery and vomiting after pediatric strabismus surgery. Acta Anaesthesiol Scand 1992; 36: 182–186.
Morton NS, Wee M, Cristie G, Gray IG, Grant IS . Propofol for induction of anaesthesia in children. A comparison with thiopentone and halothane inhalational induction. Anaesthesia 1988; 43: 350–355.
Hahnenkamp K, Hönemann CW, Fischer LG, Durieux ME, Muehlendyck H, Braun U . Effect of different anaesthetic regimes on the oculocardiac reflex during paediatric strabismus surgery. Paediatr Anaesth 2000; 10: 601–608.
Bryson HM, Fulton BR, Faulds D . Propofol. An update of its use in anaesthesia and conscious sedation. Drugs 1995; 50: 513–519.
Mackenzie N, Grant IS . Propofol for intravenous sedation. Anaesthesia 1987; 42: 3–6.
Reimer EJ, Montgomery CJ, Bevan JC, Merrick PM, Blackstock D, Popvic V . Propofol anaesthesia reduces early post-operative emesis after paediatric strabismus surgery. Can J Anaesth 1993; 40: 927–933.
Feibel RM, Guyton DL . Transient central retinal artery occlusion after posterior sub-Tenon's anesthesia. J Cataract Refract Surg 2003; 29: 1821–1824.
Frieman BJ, Friedberg MA . Globe perforation associated with subtenon's anesthesia. Am J Ophthalmol 2001; 131: 520–521.
Adams W, Morgan SJ . Diplopia following sub-Tenon's infiltration of local anesthesia. J Cataract Refract Surg 2002; 28: 1694–1697.
Kim SK, Andreoli CM, Rizzo JF, Golden MA, Bradbury MJ . Optic neuropathy secondary to sub-tenon anesthetic injection in cataract surgery. Arch Ophthalmol 2003; 121: 907–909.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Snir, M., Bachar, M., Katz, J. et al. Combined propofol sedation with sub-Tenon's lidocaine/mercaine infusion for strabismus surgery in adults. Eye 21, 1155–1161 (2007). https://doi.org/10.1038/sj.eye.6702426
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702426
Keywords
This article is cited by
-
Sub-Tenon’s anaesthesia for modern eye surgery—clinicians’ perspective, 30 years after re-introduction
Eye (2021)
-
Adjustable suture strabismus surgery
Eye (2011)
-
Anästhesie in der Ophthalmologie – Ophthalmologie in der Anästhesie
Spektrum der Augenheilkunde (2010)
