
Abstract
Purpose
To analyse the influence of baseline clinical characteristics on the outcome of verteporfin photodynamic therapy (VPDT) for neovascular age-related macular degeneration (nAMD).
Methods
A total of 1008 patients commencing VPDT for nAMD in a single UK centre entered a prospective observational study between 1999 and 2006 and were followed for 2 years. Longitudinal linear mixed-effects modelling was applied to assess the influence of baseline covariates, such as best corrected visual acuity (BCVA), contrast sensitivity (CS), age, lesion size, and lesion type, on changes of BCVA over time in patients after VPDT. A logistic regression analysis was used to analyse clinical features significantly associated with treatment failure.
Results
Study eye BCVA was significantly better on average throughout the course of treatment in patients with better baseline BCVA and CS in the study eye (P<0.001 and P<0.01, respectively) and lower age (P=0.01). Mean BCVA showed a significant reduction over time with a significant quadratic relationship between 0 and 6 months and with stabilisation between 6 and 9 months. Patients with better BCVA and worse CS at baseline, and those in whom BCVA dropped during the first 3 months of follow-up, were more likely to lose ⩾15 letters after 12 months.
Conclusions
Findings from our large longitudinal data set provide estimates of likely outcome based on baseline features and response at 3 months in patients commencing a course of VPDT for nAMD. Statistical modelling built up for this large data set can be applicable to other studies in ophthalmology research.
Similar content being viewed by others

Introduction
Neovascular age-related macular degeneration (nAMD) is the leading cause of severe visual impairment in the developed world in patients over 50 years of age.1, 2, 3 Verteporfin photodynamic therapy (VPDT) has been shown to be effective in randomised controlled clinical trials (RCTs) at reducing the likelihood of further visual loss when choroidal neovascularisation (CNV) is characterised on fundus fluorescein angiography (FA) as classic/no occult or predominantly classic.4, 5 Similar effectiveness is observed in routine clinical practise.6, 7
RCTs have shown efficacy of intravitreal therapy with pegaptanib similar to VPDT but across all angiographic lesion types.8 For ranibizumab, there was an additional benefit shown with a gain of 15 or more letters for the 0.5 mg dose of between 33.8 and 40.4% of the patients at 12 months depending on lesion subtype leading to its introduction into routine clinical practise.9, 10 However, long-term experience of anti-vascular endothelial growth factor (VEGF) therapy remains limited with uncertainty regarding ocular and systemic complications and the acceptability and feasibility of the required 4 weekly treatment regime. VPDT continues to be used as monotherapy in selected groups of patients such as those who do not adequately respond to anti-VEGF treatment or have concerns regarding an intraocular injection procedure, and in research settings as part of combined therapy protocols.11 We analysed the value of clinical features at baseline and at the first review visit in predicting the outcome of VPDT for nAMD using a large data set collected from a single treatment centre. Descriptive data on outcomes at 12 and 24 months are published elsewhere.7 We derived a statistical model to provide useful information regarding factors influencing the response to treatment.
Materials and methods
After informed consent for data collection and analysis, patients commencing a course of VPDT for nAMD at St Paul's Eye Unit, Royal Liverpool University Hospital were recruited into a prospective observational study. Patients were observed every 3 months during 2 years, reduced to every 6 months in the second year if the lesion showed clinical features of inactivation. In cases of bilateral treatment, the first treated eye was considered as the study eye.
Study procedures are described in detail elsewhere.7 In brief, best corrected visual acuity (BCVA) was measured at each visit and contrast sensitivity (CS) at alternate visits using standardised refraction and testing protocols by accredited optometrists.7 BCVA and CS were recorded as letters read at one metre on an Early Treatment Diabetic Retinopathy Study (ETDRS) logMAR chart and Pelli–Robson chart, respectively.12 Treatment was administered according to the TAP protocol4 and re-treatment guided by a locally produced protocol.6
Data were analysed using two methods. First, a linear mixed-effects model examined the relationship between baseline covariates and BCVA over time using the restricted maximum likelihood (REML) procedure. A second analysis used logistic regression to analyse explanatory variables associated with failure of treatment after 1 year. Failure was defined as a drop in absolute BCVA to below 20 letters and/or a loss of BCVA ⩾15 letters from baseline.12, 13
The study was approved by the local institutional review board and conducted within the Declaration of Helsinki guidelines.
Results
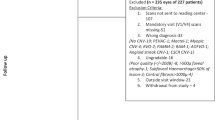
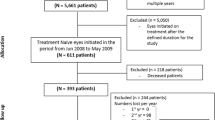
Of 1438 patients referred between November 1999 and October 2006 for possible treatment, 1008 met the eligibility criteria,7 were recruited for the study and commenced their course of VPDT. The study population was 706 at 12 months and 386 at 24 months, respectively. Distribution of patients is shown in Figure 1.

Flow chart illustrating distribution during follow-up of 1008 patients commencing a course of photodynamic therapy for neovascular age-related macular degeneration.
At baseline, the mean age was 77.2 years (range 47–102, SD 7.5) and 540 (54%) were women. The majority of patients had classic no occult (735 (72.9%)) or predominantly classic CNV (218 (21.6%)), with a small number of other lesion types (minimally classic: 41 (including RAP) and other: 14 (including PCV and occult/no classic)). Mean greatest linear diameter (GLD) at baseline was 3247 μm (range 322–7380, SD 1492).
Mean BCVA (SD) was 48.4 letters (11.1) at baseline falling to 38.3 (17.9) at 12 months. Mean CS (SD) was 21.5 (6.8) at baseline and it remained constant at 12 months with values 21.5 (8.1). Mean total number of treatments (SD) was 2.91 (1.2) in year 1 and 0.54 (0.8), with 63% of the patients having no treatment, in year 2.
The change in mean BCVA over time is shown in Figure 2 together with the 5th, 10th, 25th, 75th, 90th, and 95th percentiles. After an initial fall, the mean BCVA stabilised between 6 and 9 months. There was a wide variation in BCVA curves of individual study eyes.

Mean visual acuities over 24 months follow-up of 1008 patients undergoing photodynamic therapy for neovascular age-related macular degeneration (thick black line). The 5th, 10th, 25th, 75th, 90th, and 95th percentiles are also plotted.
Longitudinal mixed-effects analysis
The results of the longitudinal mixed-effects analysis are summarised in Table 1. The analysis was performed on data from 829 patients after excluding those patients for whom the values of one or more baseline covariates were missing (missing observations were considered to be missing completely at random). A random effect term with intercept and time slope was included in the model to account for a different baseline value and change of BCVA over time for each patient. A continuous auto-regression structure with parameter estimate phi=0.58 was chosen to model the within individual correlation based on the best-fitting-model (BIC criteria).
The statistical analysis revealed that changes in BCVA of the study eye were significantly associated with the value of BCVA at baseline (as one would expect due to their inherent correlation), as well as with the baseline covariates CS, age, and lesion size. In particular, BCVA was significantly better on average throughout the course of treatment in patients with better BCVA of the study eye at baseline (P<0.001), better CS of the study eye at baseline (P=0.003), lower age (P=0.01), and smaller lesion size (P=0.003).
Large values of BCVA at baseline were associated with large values of BCVA at any time point. However, patients with larger values of BCVA tended to lose more letters as indicated by the negative linear slope −0.04. For example, if at baseline patient A had 20 letters more in BCVA than patient B, the negative linear term indicates that patient A would tend to lose approximately 0.8 letters more per month than patient B. The positive quadratic slope (0.0011) implies that the loss of letters because of large values of BCVA at baseline becomes less important as time increases. The opposite effect was observed with CS: patients with larger values of CS at baseline tended to gain more letters over time (positive linear slope equal to 0.05). For example, if the CS of patient A is at baseline 20 letters greater than patient B, patient A will tend to gain approximately one letter more than patient B per month. The negative value for the quadratic slope (−0.0013) indicates that this effect becomes less strong over time.
Table 1 also shows that older patients and those with larger values of lesion size tend to show a worse outcome with more letters of BCVA lost, although the size of these effects was small and was not clinically significant. Finally, lesion type classified as predominantly classic showed a slightly better outcome than classic/no occult. BCVA of the fellow eye at baseline and gender were not statistically significant and do not seem to influence BCVA changes over time.
We also analysed whether the number of treatments was significantly associated with changes in visual acuity. This question was addressed by taking into account that patients had different lengths of follow-up and no significant association was detected.
Logistic regression analysis
Table 2 shows the result of the logistic regression analysis for treatment failure after 1 year as a function of baseline BCVA, CS, age, and lesion type. Patients with large values of BCVA at baseline were more likely to experience treatment failure (P<0.001). In particular, the odds of treatment failure increased by 65% for every 10 letters increase of BCVA at baseline (odds ratio (OR): exp(10*0.05)=1.65, P<0.001). This effect can be explained by taking into account the definition for treatment failure adopted (see Materials and methods section) and that patients with larger BCVA at baseline tend to lose more letters as deduced from the longitudinal analysis. In addition, patients with low values of CS at baseline were more likely to experience treatment failure (P<0.001). When taking into account CS at baseline, the odds of treatment failure decreases approximately three times for every 10 letters increase of CS at baseline (OR: exp(10*(−0.10))=0.37, P<0.001). Younger patients and patients with predominantly classic CNV were less likely to fail treatment (both P=0.02, see Table 2).
Change in BCVA at 3 months
To analyse the effect of change in BCVA at the first follow-up visit, the proportions of patients maintaining vision (<15 letters lost and BCVA⩾20 letters) at 12 months was calculated as a function of BCVA at baseline and of change of BCVA at 3 months. Both variables were segregated in ordinal steps as shown in Table 3.
As expected, because of the mathematical correlation, as the number of letters lost at first follow-up increased there was a greater chance of patients experiencing treatment failure at 12 months. The proportion of patients experiencing a treatment failure was only 20.8% (82/394) if ⩽5 letters were lost at 3 months compared with 79.8% (95/119) if 15 or more were lost at 3 months. The threshold change in BCVA at 3 months to give a 70% chance of no treatment failure was −15 letters.
Discussion
Our results provide useful information regarding the influence that baseline clinical features have on change in visual function over time in patients undergoing VPDT. The mixed-effects linear regression model applied here shows that patients with better BCVA and CS at baseline have a better outcome and that these findings are both clinically and statistically significant.
Our findings can be illustrated for the aid of clinical interpretation from the model coefficients shown in Table 1. For each 10 letters of better BCVA at baseline (two lines on an ETDRS chart or 0.2 logMAR) there was, on average, 5.3 letters better outcome in BCVA in the study eye after 12 months (where 5.3=10*(0.85−0.04*12+0.0011*122)). Patients with better BCVA at baseline experienced greater loss of BCVA over time as shown by the negative slope and this relationship was statistically significant. Therefore, for every 10 letters better BCVA at baseline there was, on average, a 4.7 letter greater loss in BCVA at 12 months. This appears to suggest that VPDT is of less benefit for patients with better levels of baseline vision and is supported by our patients final BCVA being limited to a relatively small range of absolute values. Patients with lower BCVA at the commencement of therapy are likely to have more longstanding and advanced disease. PDT may be of greater benefit at this stage when neovascular lesions are more established and the biological effect of vessel closure is more relevant.
Our results on the relationship between change in vision at 3 months and outcome at 12 months show that the initial response to VPDT can give some information regarding the final outcome. There was a 70% probability of no treatment failure in our cohort if BCVA had dropped <15 letters at 3 months. Loss of ⩾15 letters at 3 months has been termed by us as ‘primary non-response’ and indicates that clinicians should consider switching to an alternative treatment option. Our results suggest that only a small proportion of patients who have lost 15 or more letters at month 3 benefit from continued treatment. For such patients alternative treatment strategies should therefore be considered at that stage.
In contrast to the findings of better BCVA being predictive of greater visual loss, there was an inverse relationship between CS and drop in BCVA. On average, for each six letters better CS at baseline (two triplets on the Pelli–Robson chart) there was a 6.8 letter gain in BCVA over 12 months (where 6.8=10*(0.27+0.05*12−0.0013*122)). Our finding of a better CS at baseline being associated with better BCVA during follow-up raises questions regarding the differential predictive effect of different types of visual function. Our findings, supported by others,14, 15, 16, 17 suggest that CS should be used to a greater extent in assessing the efficacy of treatment of AMD.
CS arises from a summation of input from receptive fields of ganglion cells, which are further processed in the lateral geniculate nucleus.18 The photoreceptor origin of these fields is likely to extend laterally beyond the lesion boundary in nAMD. Patients with better CS at baseline may have a healthier retina surrounding the lesion, and consequently, better anatomical and functional reserve allowing a better response to therapy, either with VPDT or other treatment modalities. It is also possible that better CS may be an indicator of a less aggressive lesion more likely to respond to treatment.
Older patients experienced a worse outcome. For example, for each 10-year increment in age, BCVA was on average 1.6 letters worse at 12 months. However, this effect was not considered to be clinically significant despite being statistically significant.
The relationship between BCVA and CS at baseline and changes of BCVA over time was similar to the results observed in the TAP study indicating that our findings could be generalised to patients receiving VPDT in routine clinical practise.
The statistical longitudinal model we derived provides novel information regarding the linear and quadratic changes of BCVA over time and the effect that values of BCVA and CS at baseline have on these changes. Missing data has been assumed to be lost completely at random and although we expect that the absence of these data has not affected the main findings, a more complex statistical model in which missing values are recovered using the existing data set is under investigation.
The results of VPDT observed in our cohort and in RCTs are generally inferior to those reported with ranibizumab therapy in the ANCHOR trial.9 However, some groups of patients cannot manage the frequent injections required with anti-VEGF therapy. For these patients in whom 50% or more of their lesion comprises classic CNV it would appear reasonable to consider VPDT to reduce the frequency of visits and treatments. Our findings indicate that this is particularly applicable in patients with lower BCVA but better CS at baseline. At the 3 month follow-up visit, clinicians may wish to use our results to recommend switching to another therapy if BCVA has dropped by more than 15 letters. Various combinations of anti-VEGF therapy with VPDT are currently being analysed. Our results provide a reference point for the selection of VPDT therapy for these patients.

References
Klein R, Klein BE, Linton KL . Prevalence of age-related maculopathy: the Beaver Dam Eye Study. Ophthalmology 1992; 99: 933–943.
Vingerling JR, Dielemans I, Hofman A, Grobbee DE, Hijmering M, Kramer CF et al. The prevalence of age-related maculopathy in the Rotterdam study. Ophthalmology 1995; 102: 205–210.
Bressler NM, Bressler SB, Fine SL . Age-related macular degeneration. Surv Ophthalmol 1988; 32: 375–413.
TAP Study Group. Photodynamic therapy of subfoveal choroidal neovascularisation in age-related macular degeneration with verteporfin: one-year results of 2 randomised clinical trials. TAP report 1. Arch Ophthalmol 1999; 117: 1239–1245.
TAP Study Group. Photodynamic therapy of subfoveal choroidal neovascularisation in age-related macular degeneration with verteporfin: two-year results of 2 randomised clinical trials. TAP report 2. Arch Ophthalmol 2001; 119: 198–207.
Barnes RM, Gee L, Taylor S, Briggs MC, Harding SP . Outcomes in verteporfin photodynamic therapy for choroidal neovascularisation – ‘beyond the TAP study’. Eye 2004; 18: 809–813.
Murjaneh M, García-Fiñana M, Mahmood S, Lenfestey PM, Taylor SA, Pearce IA et al. Observational prospective study of the effectiveness in routine clinical practice of verteporfin photodynamic therapy in patients with neovascular age-related macular degeneration. Br J Ophthalmol 2009; 93 (4): 468–473.
Gragoudas ES, Adamis AP, Cunningham Jr ET, Feinsod M, Guyer DR, VEGF Inhibition Study in Ocular Neovascularization Clinical Trial Group. Pegaptanib for neovascular age-related macular degeneration. N Engl J Med 2004; 351 (27): 2805–2816.
Brown DM, Kaiser PK, Michels M, Soubrane G, Heier JS, Kim RY et al, ANCHOR Study Group. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 2006; 355 (14): 1432–1444.
Rosenfeld PJ, Brown DM, Heier JS, Boyer DS, Kaiser PK, Chung CY et al, MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 2006; 355 (14): 1419–1431.
Heier JS, Boyer DS, Ciulla TA, Ferrone PJ, Jumper JM, Gentile RC et al, FOCUS Study Group. Ranibizumab combined with verteporfin photodynamic therapy in neovascular age-related macular degeneration: year 1 results of the FOCUS Study. Arch Ophthalmol. 2006; 124 (11): 1532–1542.
Early Treatment Diabetic Retinopathy Study Research Group. Early Treatment Diabetic Retinopathy Study design and baseline patient characteristics: ETDRS Report Number 7. Ophthalmology 1991; 98: 741–756.
Macular Photocoagulation Study Group. Argon laser photocoagulation for senile macular degeneration. Results of a randomized clinical trial. Arch Ophthamol 1982; 100: 912–918.
Bansback N, Czoski-Murray C, Carlton J, Lewis G, Hughes L, Espallaraques M et al. Determinants of health related quality of life and health state utility in patients with age related macular degeneration: the association of contrast sensitivity and visual acuity. Qual Life Res 2007; 16 (3): 533–543.
Mones J, Rubin GS . Contrast sensitivity as an outcome measure in patients with subfoveal choroidal neovascularisation due to age-related macular degeneration. Eye 2005; 19 (11): 1142–1150.
Owsley C, Sekuler R, Boldt C . Aging and low-contrast vision: face perception. Invest Ophthalmol Vis Sci 1981; 21 (2): 362–365.
Ziemssen F, Lüke M, Bartz-Schmidt KU, Gelisken F . Time-dependent effects on contrast sensitivity, near and distance acuity: difference in functional parameters? (prospective, randomized pilot trial of photodynamic therapy versus full macular translocation). Graefes Arch Clin Exp Ophthalmol 2008; 246 (5): 653–659.
Chalupa LM, Werner JS (eds). The Visual Neurosciences. MIT Press: Cambridge, Massachusetts, 2003.
Acknowledgements
We acknowledge funding from The Foundation for the Prevention of Blindness and from the St Paul's Eye Unit at the Royal Liverpool University Hospital. We are grateful to Professor Paula Williamson for her useful input during earlier discussions on this study. Data from some of the patients reported in this paper observed between May 2004 and September 2007 have contributed to a larger data set in the Verteporfin Photodynamic Cohort Study, funded by National Coordinating Centre for Health Technology Assessment (NHS Clinical Trials), ref 07/36/01.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict in interest.
Rights and permissions
About this article
Cite this article
García-Fiñana, M., Murjaneh, S., Mahmood, S. et al. Baseline clinical measures and early response predict success in verteporfin photodynamic therapy for neovascular age-related macular degeneration. Eye 24, 1213–1219 (2010). https://doi.org/10.1038/eye.2009.319
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2009.319
