
Abstract
Purpose
To compare the development of posterior capsule opacification (PCO) for idiopathic epi-retinal membrane cases between 20- and 23-gauge phacovitrectomy.
Methods
Cataract surgery of phacoemulsification with the SA60AT implantation and 20- or 23-gauge vitrectomy was performed for 20 patients in both groups. Cataract surgery alone was performed for 50 patients as the control. The PCO density values were measured using Scheimpflug video photography at 1 week, 1, 3, 6, 12, 18, and 24 months after surgery. The number of eyes that required Nd:YAG laser capsulotomy was also examined.
Results
The mean PCO value in the 20-gauge phacovitrectomy group increased significantly with time (P<0.001), whereas those in the 23-gauge phacovitrectomy group and the cataract surgery group did not show any significant change. Furthermore, the PCO value in the 20-gauge phacovitrectomy group was significantly greater than that in the 23-gauge phacovitrectomy group at 6, 12, 18 (P<0.05), and 24 months (P<0.01) after surgery. The PCO value in the 23-gauge phacovitrectomy group was significantly greater than that in the cataract surgery group 24 months after surgery (P<0.05). The rate of capsulotomy in the 20-gauge phacovitrectomy group was significantly higher than that in the cataract surgery group (P=0.007), whereas there was no significant difference between the 23-gauge phacovitrectomy group and the cataract surgery group.
Conclusion
PCO rate in eyes with the 23-gauge phacovitrectomy was lower than in those with the 20-gauge phacovitrectomy, and PCO rate even in the 23-gauge phacovitrectomy was higher than in those with cataract surgery.
Similar content being viewed by others

Introduction
In cases of coexistent cataract and macular diseases, small-incision phacoemulsification with implantation of foldable intraocular lenses (IOLs) combined with pars plana vitrectomy (phacovitrectomy) has become a preferable procedure, because 75–80% of eyes developed clinically significant cataract within several years after vitrectomy, requiring subsequent cataract surgery. The added benefit of these combined procedures includes better visualization of the posterior segment during surgery, and offers earlier visual rehabilitation, and reduces the total cost of surgery.1
Posterior capsule opacification (PCO) is still the most common complication of primary cataract surgery.2 The rate of PCO following 20-gauge phacovitrectomy has been observed frequently, with reports ranging from 10.3 to 51.1%.3, 4, 5 Phacovitrectomy includes a greater number of procedural steps compared with cataract surgery. Rahman et al6 evaluated several factors contributing to PCO following phacovitrectomy, and concluded that using short-acting gas tamponade and avoiding postoperative posturing may help lower PCO rates. However, those procedures are required in some retinal disease, such as rhegmatogenous retinal detachment or macular hole. Accordingly, the difference between the characteristic of patients and the kinds of retinal disease can affect the resulting outcome; therefore, the selection bias should be minimized in a study of PCO development in phacovitrectomy.
In this study, we evaluated the development of PCO only in idiopathic epi-retinal membrane (ERM) cases without additional procedures such as laser photocoagulation or gas tamponade to minimize the selection bias among 20-gauge, 23-gauge phacovitrectomy, and cataract surgery alone in implanting a same IOL SA60AT.
Patients and methods
This single-center prospective study was conducted at the Department of Ophthalmology, Toyama Prefectural Central Hospital. Surgery was carried out based on the approval of the Institutional Review Board and the ethical standards established by the Declaration of Helsinki, and informed consent was obtained from all patients. Data were collected on vitrectomy cases performed using a 20-gauge system between August and December 2005, and vitrectomy cases performed using a 23-gauge system between January and April 2006, and cases performed using phacoemulsification between July 2006 and August 2006 by a single surgeon (TI).
All patients were followed for 24 months after surgery. Exclusion criteria were: ocular pathology other than senile cataract and idiopathic ERM, prior history of intraocular surgery, a pupillary diameter <6.0 mm after full dilation, uveitis, retinitis pigmentosa, pseudoexfoliation syndrome glaucoma, axial length longer than 25 mm or shorter than 21 mm, and performance of additional procedures such as laser photocoagulation and gas tamponade during phacovitrectomy. The continuous curvilinear capsulorrhexis (CCC) was sized to ensure complete overlap of the IOL optic during surgery. Cases with intraoperative complications (eg, incomplete CCC, posterior capsular rupture), and/or with postoperative complications (eg, iris synechia), were excluded from this study. Incomplete CCC included anterior capsular crack formation and incomplete overlap of the IOL optic.
Degree of inflammation
The degree of anterior segment postoperative inflammation was graded qualitatively by slit-lamp examination adapted from Summed Ocular Inflammation Score (SOIS). Each patient was given a clinical inflammation assessment score:
-
Anterior chamber cell count: 0=no cells, 0.5=1–5 cells, 1=6–15 cells, 2=16–25 cells, 3=26–50 cells, 4>50 cells.
-
Anterior chamber flare: 0=absent, 1=very slight (barely detectable), 2=moderate (iris and lens clear), 3=marked (iris and lens hazy), 4=intense (fibrin clot).
Assignment of IOLs
Each eye received a hydrophobic acrylic 1-piece IOL (AcrySof SA60AT, Alcon Laboratories, Fort Worth, TX, USA). The SA60AT IOL has an anterior asymmetric biconvex optic with a diameter of 6.0 mm, an overall length of 13.0 mm, supporting haptics of the same soft acrylic material as the optic, and no haptic angulation (0 degrees).
Surgical technique
After administration of retrobulbar and peribulbar anesthesia (2% lidocaine hydrochloride), a half-round fornix-based conjunctival incision was created in the 20-gauge phacovitrectomy group. A 3-mm wide self-sealing sclerocorneal tunnel was created at 12 O’clock in all of the groups. The anterior chamber was filled with a viscoelastic material, and a 5.0–5.25 mm CCC, slightly smaller than the IOL optic diameter, was made to attain circumferential 360-degree capsulorhexis-IOL overlap. Thorough hydrodissection, phacoemulsification of the nucleus, and aspiration of the residual cortex was performed. The wound was not enlarged and the SA60AT IOLs were inserted in the capsular bag using the Monarch II injector (Alcon Laboratories). Sutures were not used to close the sclerocorneal tunnel incision. After making 3 scleral port (trans-conjunctiva scleral port with trocars in the 23-gauge phacovitrectomy group), vitrectomy and ERM peeling without staining were performed. Each sclerotomy was then closed with a 7.0 vicryl suture in the 20-gauge phacovitrectomy group. No leakage from sclerotomies was obtained in any case after intracameral BSS infusion in the both groups. Finally, the conjunctival wound was sutured in the 20-gauge phacovitrectomy group. Suturing of the scleral ports and the conjunctiva was not needed in the 23-gauge phacovitrectomy group. Postoperatively, all patients received similar routine medication, comprising topical application of diclofenac sodium, 0.1% fluorometholone and levofloxacin administered four times daily for 1 month.
Measurement of PCO density
The PCO density value was measured using Scheimpflug video photography7(EAS-1000, NIDEK, Gamagori, Japan) at 1 week, 1, 3, 6, 12, 18, and 24 months after surgery. The PCO density value was determined as below. Scheimpflug slit images of the IOL were taken at the 0°, 45°, 90°, and 135° meridians after full dilation of the pupil. The highest quality image was transferred to an image analysis computer. Axial densitometry was used to measure the average scattering light density of the central 3.00 × 0.25 mm area of the posterior capsule, and of the central 3.00 × 0.25 mm area of the anterior IOL surface. The PCO density value was expressed in computer compatible tape steps (CCT) in which scattering light density obtained by the densitometry dividing the range from 0 to 255 (256 steps). The PCO density value in the cross-sectional image was determined by subtracting the scattering light density of the anterior IOL surface area from that of the posterior capsule area. The PCO values of the four meridians were then averaged and considered to represent the PCO value.
The rate of Nd:YAG laser capsulotomy
The number of eyes that required Nd:YAG laser capsulotomy was examined using Kaplan–Meier survival analysis. Nd:YAG laser capsulotomy was performed when an eye lost two or more decimal lines of acuity or when the patient complained of blurred vision. For those patients who underwent Nd:YAG laser capsulotomy, the EAS-1000 value and visual acuity just before Nd:YAG laser capsulotomy were used for further statistical analysis.
Statistical analysis
Normality of data distribution was assessed using the Kolmogorov–Smirnov test. Differences in the degree of IOL movement that showed a normal distribution were compared using the unpaired t test. Continuous variables without a normal distribution were compared using the Mann–Whitney U test. A repeated-measures analysis of variance was used to compare differences at the various examinations. Differences with a P-value less than 0.05 were considered statistically significant.
Results
Of the 111 patients that underwent surgery, 21 patients were excluded based on the exclusion criteria during and after surgery. The reasons for the exclusions were incomplete CCC (ie, anterior capsular crack formation and/or incomplete overlap of the IOL optic) (17 patients), posterior capsular rupture (2 patients), and laser photocoagulation and gas tamponade (2 patients). Accordingly, 20, 20, and 50 patients were enrolled in the 20-gauge phacovitrectomy group, the 23-gauge phacovitrectomy group, and the cataract surgery group, respectively. All procedures were uneventful in all of the groups. There was no case of postoperative hypotony or endophthalmitis.
The mean age of the patients was 65.1±7.9 years (range 54–78 years) in the 20-gauge phacovitrectomy group, 67.0±6.4 years (range 60–81 years) in the 23-gauge phacovitrectomy group, and 68.3±6.5 years (range 56–79 years) in the cataract group. The mean axial length of the patients was 23.15±1.06 mm (range 21.53–24.56 mm) in the 20-gauge phacovitrectomy group, 23.41±1.27 mm (range 21.65–24.66 mm) in the 23-gauge phacovitrectomy group, and 23.05±0.99 mm (range 21.13–24.89 mm) in the cataract surgery group (see Table 1). There was no difference in gender among the groups.
Figure 1 shows the changes in mean PCO values in the groups. The mean PCO value in the 20-gauge phacovitrectomy group increased significantly with time (P<0.001), whereas that in the 23-gauge phacovitrectomy group and the cataract surgery group did not show any significant change. Furthermore, the PCO value in the 20-gauge phacovitrectomy group was significantly greater than that in the 23-gauge phacovitrectomy group, 6, 12, 18, and 24 months after surgery, and the PCO value in the 23-gauge phacovitrectomy group was significantly greater than that in the cataract surgery group, 24 months after surgery (Figure 2).

Changes in mean (SD) posterior capsule opacification (PCO) value in the 20- and 23-gauge phacovitrectomy and cataract surgery groups. The PCO value in 20-gauge phacovitrectomy group increased significantly (P<0.001), whereas the change in the PCO value was not significant in the 23-gauge phacovitrectomy or the cataract surgery group. The mean PCO value in the 20-gauge phacovitrectomy group was significantly greater than that in the 23-gauge phacovitrectomy group, 6, 12, 18, and 24 month after surgery. Also, the PCO value in the 23-gauge group was significantly greater than that in the cataract surgery group, 24 months after surgery.

Representative photographs of eyes following (a) 20-, (b) 23-gauge phacovitrectomy and (c) cataract surgery showing the development of PCO.
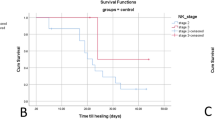
Three (15%) in the 20-gauge phacovitrectomy group, 2 (10%) in the 23-gauge phacovitrectomy group, and 1 (2%) in the cataract surgery group required Nd:YAG laser capsulotomy within 24 months after surgery (Figure 3). Kaplan–Meier survival analysis demonstrated that the rate of capsulotomy in the 20-gauge phacovitrectomy group was significantly higher than that in the cataract surgery group (P=0.007, Mantel–Cox log-rank test), whereas there was no significant difference between the 23-gauge phacovitrectomy group and the cataract surgery group.

Kaplan–Meier survival plots of the two groups for eyes not requiring Nd:YAG laser posterior capsulotomy. The survival curve in the 20-gauge phacovitrectomy group was significantly worse compared with the cataract surgery group (P=0.007, Mantel–Cox log-rank test), whereas there was no significant difference between the 23-gauge phacovitrectomy group and the cataract surgery group.
Figure 4 shows the ocular inflammation score in the groups. The mean SOIS score in the 20-gauge phacovitrectomy group was significantly greater than that in the 23-gauge phacovitrectomy group and in the cataract surgery group, 1 and 7 days after surgery (P<0.05).

Mean SOIS at 1, 7, and 30 days following surgery. The mean SOIS score in the 20-gauge phacovitrectomy group was significantly greater than that in the 23-gauge phacovitrectomy group, 1 day after surgery and that in the cataract surgery group, 1 and 7 days after surgery.
Conclusion
With the tremendous advances in surgical techniques and the improvement of IOLs, the incidence of PCO has been reduced greatly. However, PCO remains one of the most common complications after cataract surgery. Numerous investigators have revealed three factors predominantly contributing to the incidence and degree of PCO: surgical technique,8, 9, 10, 11 IOL design,12, 13 and IOL material. In the present study, the same IOL SA60AT was implanted in all of the cases, indicating surgical procedure (technique) is only difference among the groups.
Vitrectomy involves various complicated procedures and there are many variables that can be associated with the development of PCO compared with cataract surgery. These include occurrence of intraoperative/postoperative complications, usage of long acting gas tamponade, and postoperative posturing.6 Accordingly, the difference between the characteristic of patients and the kinds of retinal disease can affect the resulting outcome; therefore, the selection bias should be minimized in a study of PCO development in phacovitrectomy. There have been a few reports regarding the development of PCO following phacovitrectomy.3, 4, 6, 14 However, those studies included several kinds of disease and used various procedures, including gas tamponade, indicating that those results could be affected by selection bias. Thus, in this report, the same three procedures were performed for each ERM case; cataract surgery, core vitrectomy, and ERM peeling. A trim of the peripheral vitreous was not performed in order to avoid ocular inflammation. Also, in order to avoid unnecessary pressure on the capsular bag, gas tamponade was not performed. For this study, cases that were complicated by additional procedures and diagnoses other than ERM were excluded. This is why the number of phacovitrectomy groups is relatively small (20 eyes in each phacovitrectomy group); because the candidates for this study was narrow in order to minimize selection bias.
To our best knowledge, this is the first report quantifying PCO in phacovitrectomy using non-qualitative means (EAS-1000, Scheimpflug camera). The incidence of PCO following 23-gauge phacovitrectomy in this study is lower than the 20-gauge phacovitrectomy. Also, selection bias was minimized in our study. Therefore, these results can be attributed to the small-sized vitrectomy instrument trauma (no conjunctival peritomy, smaller instruments, and no scleral sutures), because the postoperative intraocular inflammation was less in smaller gauge phacovitrectomy. Postoperative inflammation is linked to PCO development and has been extensively studied in uveitic eyes undergoing cataract surgery, with generally high rates of incidence being reported (ranging from 10 to 96%).15, 16
On the other hand, the incidence of PCO following 23-gauge phacovitrectomy in this study is higher than cataract surgery. Previous studies have reported that PCO developed more frequently after phacovitrectomy than after cataract surgery alone. Toda et al5 found that the PCO rate was 4.2% in the cataract surgery group, and 10.3% in the phacovitrectomy group. Mochizuki et al3 reported that the PCO rate was 17.9% in phacovitrectomy group. In the present study, because a relatively less traumatic vitrectomy was performed, the procedure does not seem to cause strong inflammation and actually the postoperative intraocular inflammation showed no significant differences between the 23-gauge phacovitrectomy and the cataract surgery group. However, the incidence of PCO in the 23-gauge phacovitrectomy is still higher. Nishi et al17 concluded that capsular bend formation is the key to understanding how some IOLs reduce the incidence of PCO. Both the sharpness of the bend and the speed of its formation are important factors. As there is little posterior pressure in eyes with no vitreous, and capsular bend formation may require not only a sharp optic edge but also posterior pressure, it is possible that the IOL edge has a minimal effect in reducing PCO in phacovitrectomy.18 Also, more postoperative inflammation probably leads to lens epithelial cell migration and more extensive PCO in the phacovitrectomy.5
On the other hand, Inoue et al19 reported that a 25-gauge vitrectomy group had significantly less postoperative ocular inflammation than a 20- or a 23-gauge vitrectomy group in rabbit eyes. Accordingly, the 25-gauge phacovitrectomy might have less inflammation than the 23-gauge phacovitrectomy, resulting in no difference from cataract surgery alone in terms of development of PCO.
In conclusion, the results of this study demonstrate that the PCO rate in eyes with the 23-gauge phacovitrectomy was lower than in those with the 20-gauge phacovitrectomy, and PCO rate even in the 23-gauge phacovitrectomy was higher than that in those with cataract surgery. As this study included only ERM cases, these results may only apply to ERM cases without additional procedures, such as laser photocoagulation or gas tamponade, and may not apply to other cases involving additional procedures. Further studies are needed to examine the development of PCO between phacovitrectomy and cataract surgery alone, such as using a 25-gauge phacovitrectomy.

References
Melberg NS, Thomas MA . Nuclear sclerotic cataract after vitrectomy in patients younger than 50 years of age. Ophthalmology 1995; 102 (10): 1466–1471.
Apple DJ, Solomon KD, Tetz MR, Assia EI, Holland EY, Legler UF et al. Posterior capsule opacification. Surv Ophthalmol 1992; 37 (7): 73–116.
Mochizuki Y, Kubota T, Hata Y, Miyazaki M, Suyama Y, Enaida H et al. Surgical results of combined pars plana vitrectomy, phacoemulsification, and intraocular lens implantation. Eur J Ophthalmol 2006; 16 (2): 279–286.
Ling R, Simcock P, McCoombes J, Shaw S . Presbyopic phacovitrectomy. Br J Ophthalmol 2003; 87 (11): 1333–1335.
Toda J, Kato S, Oshika T, Sugita G . Posterior capsule opacification after combined cataract surgery and vitrectomy. J Cataract Refract Surg 2007; 33 (1): 104–107.
Rahman R, Briffa BV, Gupta A, Chinn DJ . Factors contributing to posterior capsule opacification following 23-gauge transconjunctival phacovitrectomy. Ophthalmic Surg Lasers Imaging 2011; 42 (3): 229–233.
Hayashi K, Hayashi H, Nakao F, Hayashi F . Changes in posterior capsule opacification after poly(methyl methacrylate), silicone, and acrylic intraocular lens implantation. J Cataract Refract Surg 2001; 27 (6): 817–824.
Apple DJ, Peng Q, Visessook N, Werner L, Pandey SK, Escobar-Gomez M et al. Surgical prevention of posterior capsule opacification. Part 1: Progress in eliminating this complication of cataract surgery. J Cataract Refract Surg 2000; 26 (2): 180–187.
Peng Q, Apple DJ, Visessook N, Werner L, Pandey SK, Escobar-Gomez M et al. Surgical prevention of posterior capsule opacification. Part 2: enhancement of cortical cleanup by focusing on hydrodissection. J Cataract Refract Surg 2000; 26 (2): 188–197.
Wejde G, Kugelberg M, Zetterström C . Position of anterior capsulorhexis and posterior capsule opacification. Acta Ophthalmol Scand 2004; 82 (5): 531–534.
Wren SM, Spalton DJ, Jose R, Boyce J, Heatley CJ . Factors that influence the development of posterior capsule opacification with a polyacrylic intraocular lens. Am J Ophthalmol 2005; 139 (4): 691–695.
Werner L . Biocompatibility of intraocular lens materials. Curr Opin Ophthalmol 2008; 19 (1): 41–49.
Kohnen T, Fabian E, Gerl R, Hunold W, Hütz W, Strobel J et al. Optic edge design as long-term factor for posterior capsular opacification rates. Ophthalmology 2008; 115 (8): 1308–1314.
Roh JH, Sohn HJ, Lee DY, Shyn KH, Nam DH . Comparison of posterior capsular opacification between a combined procedure and a sequential procedure of pars plana vitrectomy and cataract surgery. Ophthalmologica 2010; 224 (1): 42–46.
Ganesh SK, Babu K, Biswas J . Phacoemulsification with intraocular lens implantation in cases of pars planitis. J Cataract Refract Surg 2004; 30 (10): 2072–2076.
Rahman I, Jones NP . Long-term results of cataract extraction with intraocular lens implantation in patients with uveitis. Eye (Lond) 2005; 19 (2): 191–197.
Nishi O, Nishi K, Akura J . Speed of capsular bend formation at the optic edge of acrylic, silicone, and poly(methyl methacrylate) lenses. J Cataract Refract Surg 2002; 28 (3): 431–437.
Nishi O, Nishi K, Osakabe Y . Effect of intraocular lenses on preventing posterior capsule opacification: design versus material. J Cataract Refract Surg 2004; 30 (10): 2170–2176.
Inoue Y, Kadonosono K, Yamakawa T, Uchio E, Watanabe Y, Yanagi Y et al. Surgically-induced inflammation with 20-, 23-, and 25-gauge vitrectomy systems: an experimental study. Retina 2009; 29 (4): 477–480.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Iwase, T., Oveson, B. & Nishi, Y. Posterior capsule opacification following 20- and 23-gauge phacovitrectomy (posterior capsule opacification following phacovitrectomy). Eye 26, 1459–1464 (2012). https://doi.org/10.1038/eye.2012.193
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2012.193
