
Abstract
Purpose
To investigate the incidence and risk factors for acute rhinosinusitis (ARS) following endoscopic dacryocystorhinostomy (EnDCR).
Methods
Retrospective single-surgeon interventional case series, including 196 consecutive patients undergoing 203 endonasal DCR, with clinical and radiological evidence of nasolacrimal duct or common canalicular obstruction. Pre-operative lacrimal and sinonasal clinical assessment and imaging, intraoperative endoscopic video recording, and post-operative clinical and endoscopic findings were analysed for cases of ARS occurring within the first 4 weeks following DCR among patients with and without a past history of chronic rhinosinusitis (CRS). Surgical complications and outcomes at 12 months and management of ARS are reported.
Results
Three patients (1.5%) developed ARS within the first 5 post-operative days, none of which had experienced peri-operative complications and all had a past history of CRS. The rate of CRS in this cohort of 196 patients was 10.2% (n=20), of which 15% (n=3) developed ARS, although none had symptoms of CRS at the time of surgery; one had undergone previous sinus surgery. Presenting symptoms of ARS included facial pain, tenderness over the affected sinus, and nasal discharge; all patients responded to oral antibiotic therapy.
Discussion
The rate of ARS following EnDCR was 1.5%. In those with a prior history of CRS, it was 15% (P=0.009). ARS developed within the first post-operative week among patients with a past history of CRS, who were asymptomatic at the time of surgery, and responded to oral antibiotics. CRS may be a risk factor for the development of post-operative ARS.
Similar content being viewed by others


Introduction
Primary acquired nasolacrimal duct obstruction (PANDO) is a common ophthalmic complaint, and chronic rhinosinusitis (CRS) possibly affects up to 16% of the adult population;1 the two may therefore coexist. As the lacrimal system is anatomically related to the nasal mucosa, NLDO may occur as a direct consequence of rhinologic or sinus disease.
The occurrence of post-operative acute rhinosinusitis (ARS) following routine dacryocystorhinostomy (DCR) has not been widely reported; with rates of 2% for acute maxillary sinusitis2 and 0.3–2% for frontal sinusitis recorded in retrospective series.2, 3
The purpose of the present study was to investigate the incidence of postoperative ARS in a cohort of patients undergoing endoscopic transnasal DCR and report on their clinical presentation, management, and surgical outcomes.
Materials and methods
This was a retrospective analysis of data collected as part of a prospective study designed to ascertain the rate of canalicular patency without intubation.4 As part of the study, secondary outcome measures included the rate of post-DCR ARS, based on a rate of 5% and an a priori hypothesis that there was no difference in the rate of ARS among patients with and without a history of CRS. A total of 196 consecutive patients with symptomatic PANDO and common canalicular obstruction were prospectively enrolled into this non-randomised, non-comparative, interventional case series to investigate the incidence of post-operative ARS following powered endoscopic DCR (EnDCR). Inclusion criteria were all cases ≥18 years undergoing EnDCR by a single surgeon (DS) with a diagnosis of PANDO or stenosis or common canalicular obstruction. The diagnosis was made clinically by syringing and confirmed radiologically in all cases using dacryocystography and dacryoscintillography, except in patients with a clinically refluxable mucocele or history of recent dacryocystitis. No external DCRs were performed during this period. Patients undergoing revision EnDCR were excluded.
Written informed consent was obtained from all patients. Patients underwent a standard pre- and post-operative lacrimal assessment of eyelids, slit lamp examination of the puncta, ocular surface and tear film, endoscopic examination of the nasal cavity, and syringing of the lacrimal apparatus. Epiphora was subjectively graded with Munk scores5 obtained pre- and post-operatively. Complete success was defined as Munk score of 0 or 1, partial success was defined as Munk score of 2, and failure was defined as Munk score of 3 or 4.
A history of sinonasal disease, allergic rhinitis, previous sinus, and facial surgery were specifically obtained. CRS was defined as having nasal blockage and discharge for >12 consecutive weeks with either mucosal thickening on computed tomography (CT) scan or a polyp or mucopus on intranasal examination.6 This diagnosis was recorded if established from an ENT review or if the diagnostic criteria for CRS were fulfilled on pre-operative assessment.
The use of silicone intubation and performance of a septoplasty or turbinectomy were documented and reviewed from intraoperative endoscopic video recordings. Patients were routinely followed up at 4 weeks and 12 months post-operatively. A diagnosis of ARS was made on the basis of purulent nasal drainage (anterior, posterior, or both), accompanied by nasal obstruction, facial pain-pressure-fullness, or both of <4 weeks duration.6 All patients were questioned regarding the presence of these symptoms in the post-operative period at the 4-week review unless they had presented earlier. Patients with symptoms of ARS underwent nasal endoscopy and a CT scan and were commenced on oral antibiotics and a topical nasal decongestant.
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research.
Statistical methods
Differences in the rate of ARS in the study cohort among those with and without a history of CRS were calculated using a two-by-two contingency table using the Fisher’s exact test. Statistical anlyses were performed using Sigmaplot version 12.5 for Windows (Systat Software, Inc., San Jose, CA, USA).
Surgical technique
All the surgical procedures were carried out by a single surgeon (DS). The EnDCR was performed under general anaesthesia or local anaesthesia with sedation using a modification of the powered EnDCR technique previously described by Wormald,7 achieving complete exposure of the lacrimal sac and apposition of nasal and lacrimal mucosa. Where membranectomy or trephination was performed, the patient was intubated with O’Donohue silicone tubes (BD Visitec DCR Set; Beaver-Visitec International, Franklin Lakes, NJ, USA) for approximately 3 months. Post-operative nasal packing was not routinely performed. Post-operative instructions included daily nasal douching with a saline spray and avoidance of nose blowing for 2 weeks. Systemic antibiotics were not routinely administered.
Results
One-hundred and ninety-six consecutive patients with symptomatic epiphora and evidence of PANDO or stenosis or canalicular obstruction underwent 203 transnasal EnDCRs (189 unilateral and 7 bilateral). The average age of all patients was 64±15 years, and 71% were female. Twenty (10.2%) patients had a past history of CRS. Patient demographics such as age and gender were comparable between those with a history of CRS and those without CRS. Table 1 summarises the clinical assessment of the two groups pre- and post DCR, including Munk scores, lacrimal imaging, and details of adjuvant surgical procedures. In all, 85% of patients with a history of CRS presented with epiphora alone, 15% with epiphora and conjunctival discharge, and none had a history of acute or chronic dacryocystitis. In contrast, 4% of patients with no history of CRS had experienced at least one episode of dacryocystitis. In all, 35% of those with CRS had undergone sinus surgery. Pre-operative CT scans were requested in 4 of the 20 patients with CRS to establish or confirm the diagnosis, and in 5 of the 20 patients, the patient’s ENT surgeon was contacted for details of their sinonasal history. The other 11 patients fulfilled the criteria on history and exam or had a documented diagnosis of CRS from an ENT surgeon. The minimum follow-up was 12 months. No patients received antibiotic prophylaxis.
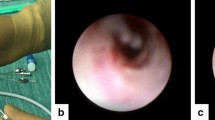
Three (1.5%) patients developed ARS within the first 5 days following DCR and presented to the surgeon within the first 11 days. Details of the three cases with ARS are presented in Table 2. All three patients had a past history of CRS that had been asymptomatic at the time surgery. All three patients had undergone uncomplicated EnDCR. Facial pain worsening with valsalva and tenderness over the affected sinus were common to all three patients, as were nasal congestion and discharge. Only one patient experienced fever, and none had symptoms of upper respiratory tract infection. A CT scan confirmed opacification of the affected sinus in each case (Figures 1, 2, 3). All three patients were treated with a 1–3-week course of oxymetazoline hydrochloride nasal spray and oral augmentin forte twice daily. The choice of antibiotic is based on randomized controlled trials of clinical outcomes in ARS, showing that penicillin or amoxicillin are comparable to broader spectrum antibiotics for initial therapy, with the potential for reduced bacterial resistance.8, 9 Antibiotics with beta-lactamase inhibition have also been shown to be more effective than those without.10 No surgical complications were experienced in these three cases; in particular, there was no disruption to the uncinate process or ethmoidal bulla in case 1; case 2 had undergone functional endoscopic sinus surgery three times in the past, the last 28 months before DCR surgery; and care was taken to ensure that the nasal mucosal flap did not extend to the anterior margin of a large maxillary antrostomy. No cases of ARS were associated with the placement of a lacrimal stent at the time of surgery or post-operative haemorrhage. The outcome of DCR surgery in all three cases with ARS was successful, with complete anatomical patency of the lacrimal drainage system at 12 months. Cases 1 and 2 had full symptom resolution by 12 months and case 3 by 32 months, following the placement of a silicon bicanalicular lacrimal stent for the management of his functional epiphora, which he has decided to keep in situ.

Case 1 coronal CT scan showing opacification of the anterior ethmoid sinuses, including those not opened during surgery.

Case 2 coronal CT scan showing extensive mucosal thickening and bony sclerosis, consistent with chronic rhinosinusitis within the maxillary sinuses and ethmoid air cells with evidence of previous sinus surgery, such as the absence of inferior turbinates.

Case 3 coronal CT scan demonstrating the opacification of the right maxillary sinus.
There was a significant difference in the rate of post-operative ARS between those with a history of CRS 15% and those without 0%, (P=0.009). There was no significant difference between the two groups in the success of DCR surgery and symptom resolution at 12 months (85% in those with CRS and 90% in those without). There were two cases of immediate post-operative epistaxis that were controlled within 30 min using ice packs in theatre recovery. Neither of these patients had a past history of CRS or developed ARS. No patients required nasal packing.
Discussion
In this study, the prevalence of CRS among the 196 patients who underwent EnDCR was 10.2%, and the overall incidence post DCR ARS was 1.5%. Among patients with a history of CRS, the incidence of ARS was 15%. Although all three cases with ARS had a positive history of CRS, none had symptoms at the time of surgery, and the development of ARS may have been purely coincidental. However, the symptoms of ARS commenced early, within the first 5 days following DCR surgery.
Nasal endoscopy confirmed oedematous nasal mucosa greater than that would be expected, following endonasal DCR, and CT scans revealed mucosal thickening and opacification of the affected sinus. In the assessment of patients with symptoms of rhinosinusitis, nasal endoscopy can identify posterior septal deviation and polyps or secretions in the posterior nasal cavity, within the middle meatus, or in the sphenoethmoidal recess. Although not performed in this study, middle meatal cultures may be obtained to direct antibiotic choice.11, 12 CT of the paranasal sinuses should be obtained in evaluating a patient with CRS or recurrent ARS. Although CT findings do not necessarily correlate with symptom severity, they offer an objective method for monitoring recurrent or chronic disease.13, 14
Mechanisms that have been suggested for the development of ARS include intraoperative trauma to middle meatal structures or placement of a lacrimal stent resulting in significant mucosal swelling and formation of adhesions. It should be noted that the vertical portion of the uncinate may overlie the posterior aspect of the lacrimal sac in 55–65% of patients,15, 16, 17 and hence elevation of the nasal mucosal flap will often extend to involve the root of the vertical portion of the uncinate process. However, damage to the maxillary ostium would require dissection posterior this level. Frontal sinusitis following DCR surgery has also been reported due to an electrocautery burn to the frontonasal duct during a middle turbinectomy, resulting in closure of the ostial mucosa.18
In our series, these mechanisms seem unlikely, as review of the intraoperative videos showed no damage to the middle meatus or frontonasal recess. Second, no cases with ARS received stents at the time of DCR. Other contributory factors could be a narrow nasal space or the presence of septal deviation; one in three of our cases with ARS underwent septoplasty. It is possible that where natural sinus ostea are already narrow from congenital or acquired causes, post-operative mucosal inflammation alone may result in closure. Infection could also have commenced at the site of surgery with secondary involvement of the sinuses, especially if there was an underlying predisposition to the development of ARS.
Mucociliary clearance is an important component of the defence mechanisms of the respiratory tracts and can be impaired by conditions such as CRS19 that affect the activity of cilia. Diminished mucociliary clearance has also been reported following both external20 and EnDCR.21, 22 Saline nasal irrigation is therefore recommended for secondary prevention of CRS, recurrent ARS, and after sinus surgery.23
Other series documenting rates of post-operative ARS of up to 2%2, 3 did not specify their diagnostic criteria, and therefore it is difficult to draw any comparisons with this series. The prevalence of CRS in this study cohort was 10.2%. Data from the National Health Interview Survey,24 which rely on patient self-reporting, state the prevalence of CRS as 14–16% in the United States. Studies using the International Classification of Diseases (ICD-9) codes report a much lower prevalence (1.96%) of CRS.25 The prevalence of CRS in this cohort may be higher than in other series because of the significant number of referrals to the senior author’s practice from ENT specialists. All surgeons performing DCR should be able to pre-operatively identify patients who may benefit from referral to a rhinologist.
In conclusion, ARS appears be an uncommon complication of DCR surgery (1.5%), and ophthalmologists should be familiar with the diagnosis and management of ARS. In addition, a history of CRS may be a risk factor because all the three cases with ARS described here had a positive history, although none had symptoms of active infection at the time of surgery. The question of whether peri-operative antibiotics might diminish the risk of post-operative ARS in these patients remains speculative in the absence of further study. The current practice of the senior surgeon is to give patients with a past history of CRS a course of prophylactic antibiotics.

References
Benninger MS, Ferguson BJ, Hadley JA, Hamilos DL, Jacobs M, Kennedy DW et al. Adult chronic rhinosinusitis: definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol Head Neck Surg 2003; 129: S1–32.
Leong SC, Macewen CJ, White PS . A systematic review of outcomes after dacryocystorhinostomy in adults. Am J Rhinol Allergy 2010; 24: 81–90.
Fayet B, Racy E, Assouline M . Complications of standardized endonasal dacryocystorhinostomy with unciformectomy. Ophthalmology 2004; 111: 837–845.
Cannon PS, Chan W, Selva D . Incidence of canalicular closure with endonasal dacryocystorhinostomy without intubation in primary nasolacrimal duct obstruction. Ophthalmology 2013; pii: S0161-6420 (13): 00038–00039.
Munk PL, Lin DT, Morris DC . Epiphora: treatment by means of dacryocystoplasty with balloon dilation of the nasolacrimal drainage apparatus. Radiology 1990; 177: 687–690.
Rosenfeld RM, Andes D, Bhattacharyya N, Cheung D, Eisenberg S, Ganiats TG et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg 2007; 137: S1–31.
Wormald PJ . Powered endoscopic dacryocystorhinostomy. Laryngoscope 2002; 112: 69–72.
Williams JW Jr, Aguilar C, Cornell J, Chiquette ED, Makela M, Holleman DR et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev 2003; CD000243.
Ahovuo-Saloranta A, Borisenko OV, Kovanen N, Varonen H, Rautakorpi UM, Williams JW Jr et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev 2008; 16: CD000243.
de Bock GH, Dekker FW, Stolk J, Springer MP, Kievit J, van Houwelingen JC . Antimicrobial treatment in acute maxillary sinusitis: a meta-analysis. J Clin Epidemiol 1997; 50: 881–890.
Benninger MS, Payne SC, Ferguson BJ, Hadley JA, Ahmad N . Endoscopically directed middle meatal cultures versus maxillary sinus taps in acute bacterial maxillary rhinosinusitis: a meta-analysis. Otolaryngol Head Neck Surg 2006; 134: 3–9.
Dubin MG, Ebert CS, Coffey CS, Melroy CT, Sonnenburg RE, Senior BA . Concordance of middle meatal swab and maxillary sinus aspirate in acute and chronic sinusitis: a meta-analysis. Am J Rhinol 2005; 19: 462–470.
Bhattacharyya T, Piccirillo J, Wippold FJ 2nd . Relationship between patient-based descriptions of sinusitis and paranasal sinus computed tomographic findings. Arch Otolaryngol Head Neck Surg 1997; 123: 1189–1192.
Kenny TJ, Duncavage J, Bracikowski J, Yildirim A, Murray JJ, Tanner SB . Prospective analysis of sinus symptoms and correlation with paranasal computed tomography scan. Otolaryngol Head Neck Surg 2001; 125: 40–43.
Fayet B, Racy E, Assouline M, Zerbib M . Surgical anatomy of the lacrimal fossa a prospective computed tomodensitometry scan analysis. Ophthalmology 2005; 112: 1119–1128.
Soyka MB, Treumann T, Schlegel CT . The Agger Nasi cell and uncinate process, the keys to proper access to the nasolacrimal drainage system. Rhinology 2010; 48: 364–367.
Woo KI, Maeng HS, Kim YD . Characteristics of intranasal structures for endonasal dacryocystorhinostomy in asians. Am J Ophthalmol 2011; 152: 491.e1–498.e1.
Wesley RE, Bond JB . Intranasal procedures for successful lacrimal surgery. Ophthal Plast Reconstr Surg 1986; 2: 153–157.
Gudis D, Zhao KQ, Cohen NA . Acquired cilia dysfunction in chronic rhinosinusitis. Am J Rhinol Allergy 2012; 26: 1–6.
Unal M, Oz O, Adiguzel U, Vayisoglu Y, Vatansever H, Görür K . Mucociliary clearance after external dacryocystorhinostomy. Clin Otolaryngol Allied Sci 2004; 29: 264–265.
Yigit O, Kirgezen T, Taskin U, Yener M . Endoscopic dacryocystorhinostomy appears to impair nasal mucociliary clearance. Ear Nose Throat J 2011; 90: E23–E27.
Okuyucu S, Akoglu E, Oksuz H, Gorur H, Dagli S . The effect of dacryocystorhinostomy on mucociliary function. Otolaryngol Head Neck Surg 2009; 140: 585–588.
Slavin RG, Spector SL, Bernstein IL, Kaliner MA, Kennedy DW, Virant FS et al. The diagnosis and management of sinusitis: a practice parameter update. J Allergy Clin Immunol 2005; 116: S13–S47.
Benson V, Marano MA . Current estimates from the National Health Interview Survey, 1995. National Center for Health Statistics. Vital Health Stat. 10(199) 1998 Available at http://www.cdc.gov/nchs/data/series/sr_10/sr10_199acc.pdf.
Shashy RG, Moore EJ, Weaver A . Prevalence of the chronic sinusitis diagnosis in Olmsted County, Minnesota. Arch Otolaryngol Head Neck Surg 2004; 130: 320–323.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This study has been presented at the Royal Australian and New Zealand College of Ophthalmologists annual meeting, 2012, Melbourne, Australia, and at the British Oculoplastic Surgeons Society Meeting In Bristol in June 2013.
Rights and permissions
About this article
Cite this article
Shams, P., Selva, D. Acute post-operative rhinosinusitis following endonasal dacryocystorhinostomy. Eye 27, 1130–1136 (2013). https://doi.org/10.1038/eye.2013.147
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2013.147
