
Abstract
Overall response rate (ORR) is commonly used as key endpoint to assess treatment efficacy of chronic graft versus host disease (cGvHD), either as ORR at week 24 or as best overall response rate (BOR) at any time point up to week 24 or beyond. Both endpoints as well as duration of response (DOR) were previously reported for the REACH3 study, a phase 3 open-label, randomized study comparing ruxolitinib (RUX) versus best available therapy (BAT). The comparison between RUX and BAT was performed on ORR and BOR using all randomized patients, while DOR was derived for the subgroup of responders only. Here we illustrate the application of the probability of being in response (PBR), a graphical method presenting simultaneously the time to first response and subsequent failure using all randomized patients. In REACH3, PBR showed an earlier time to first response, a higher probability of being in response and a longer duration of response for RUX compared to BAT. PBR is a clinically easily interpretable measurement and can serve as a novel efficacy endpoint to assess treatments for chronic graft versus host disease.
Similar content being viewed by others
Introduction
Many studies investigating the treatment of graft versus host disease (GvHD) use overall response per 2014 NIH consensus criteria as the primary efficacy endpoint [1]. The overall response rate (ORR) is defined as the proportion of patients who achieve a complete response (CR) or a partial response (PR). The overall response rate (ORR) may be reported at a fixed time point or derived from the best overall response (BOR) achieved at any time point during treatment.
ORR at week 24 was used as primary endpoint in REACH3, a randomized phase 3 study comparing ruxolitinib versus best available therapy (BAT) for glucocorticoid-refractory chronic GvHD (cGvHD), and BOR at any time point up to week 24 was used as one of the secondary endpoints [2]. Both ORR at week 24 and BOR were higher for ruxolitinib than in the control group (BAT). To investigate how long the response to treatment is maintained, the duration of response (DOR) was calculated for all patients who achieved BOR = CR or PR, results were also reported in Zeiser et al. [2]. As DOR is computed for responders only, a formal statistical test to compare DOR between the two treatment arms was not performed since such a comparison would not be based on all randomized patients. Another measure of potential clinical interest is the time to the first response, which can be either calculated for responders only (e.g., all patients who achieved BOR = CR or PR) or for all randomized patients.
In this paper, we illustrate the application of the so-called probability of being in response function (PBR function), an extension of Kaplan–Meier estimation which facilitates the simultaneous graphical representation of the time to first response and subsequent failure, i.e., combining time to first response, response rates, and DOR into one easily interpretable measure using all randomized patients. PBR was introduced by Temkin et al as a non-parametric method to estimate the response probability as a function of time [3]. Begg and Larson and Ellis et al suggested estimating the PBR from parametric models [4, 5].
Materials and methods
REACH3 study and efficacy endpoints
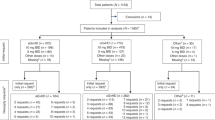
REACH3 was an open-label randomized controlled study investigating the efficacy and safety of ruxolitinib versus BAT in patients 12 years or older with glucocorticoid-refractory or dependent cGvHD. Overall, 329 patients were randomized; 165 and 164 patients were assigned to the ruxolitinib and BAT arm, respectively. All patients (or their guardian) provided informed consent. Response evaluation was performed according to the 2014 NIH consensus criteria, response assessments were made regularly (e.g., every 4 weeks up to week 24) as per study protocol [1]. ORR at week 24, defined as the proportion of patients who achieved a CR or a PR 24 weeks after randomization, was used as primary endpoint. Other efficacy endpoints included the BOR defined as proportion of patients who achieved overall response (CR or PR) at any time point up to and including week 24, the DOR which was derived for the subset of patients with BOR = CR or PR only and failure-free survival (FFS), defined as time from randomization to recurrence of underlying disease, start of new systemic treatment for cGvHD, or death, whichever came first. An overview of selected efficacy endpoints is given in supplementary material S1. More details on the REACH3 study design and results can be found in Zeiser et al. [2].
Probability of being in response function
The probability of being in response function (PBR function) suggested by Temkin can be derived from a multistate model (Fig. 1) [3]. As illustrated for seven hypothetical patients in Fig. 2, all patients are in state 0 (not in response) at baseline (=randomization date). A patient responding to treatment enters state 1 = in response at the time of the first documented response. Such patients may lose their response at a later time point and enter the absorbing state, state 2, (Pat-ID 2, 3, and 6) or remain in response at the time of the statistical analysis (Pat-ID 1), in which case they are censored in state 1. Patients who die or progress or start a new systemic cGvHD treatment or do not achieve response within 24 weeks switch from state 0 to state 2 (Pat-ID 4 and 5). For example, Pat-ID 5 might have died without response and Pat-ID 4 may not have achieved PR up to week 24. Any patient who neither reached state 1 nor state 2 (i.e., drop out before week 24 without response and without any of the events defined as state 2) would have been censored in state 0 (e.g., Pat-ID 7).

Illustration of multistate model for response status. Absorbing events were either death, start of new systemic cGvHD therapy, underlying malignancy relapse, not having achieved a response up to week 24 (non-responders only) or cGvHD progression (responders only). *Patient cannot achieve a response anymore after entering State 2.

Graphical illustration of response states overtime for seven hypothetical patients. 0, State 0, not in response; 1, State 1, in response; 2, State 2, absorbing; Pat-ID, patient ID.
Considering the day of randomization as baseline (time=0), the probability that a randomized patient is in response at a time point t can be obtained by scrolling over the time axis and assessing the state at that time point for each patient. Thus, the PBR can be calculated as a function of time by applying time-to-event methodology similar to the well-known Kaplan–Meier plot. While the Kaplan–Meier plot estimates one right-censored time-to-event variable (e.g., overall survival or duration of response) from a fixed time point (e.g., time of randomization or time of first response) for all patients, the PBR function aggregates two time-to-event variables, namely time from randomization to first response and time from first response to subsequent failure [6], more details and an illustration using the hypothetical data from Fig. 2 are provided in supplementary material S2. In order to compare PBR between treatment arms, we calculated the difference of PBR curves (ruxolitinib minus BAT) with pointwise 95% confidence intervals. All calculations were performed using R-4.1.0.
Results
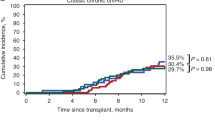
In REACH3, greater efficacy was observed on ruxolitinib versus BAT for most efficacy endpoints [2]. Summary results of the efficacy parameters are displayed in Table 1, more detailed information on the outcome of the pre-planned study endpoints is published in Zeiser et al. [2]. In addition, not reported previously, the median time to first response for all randomized patients (with non-responders censored) was 29 days (95% CI: 24 to 31 days) for ruxolitinib and 50 days (95% CI: 29 to 57 days) for BAT. A slightly earlier time to first response, a higher probability of being in response at all time points and a longer response duration for ruxolitinib than BAT is apparent from the PBR curves (Fig. 3). The higher clinical benefit of ruxolitinib is also visualized by a larger area under the curve.

Comparison of PBR for ruxolitinib (blue) versus BAT (orange) in REACH3. Solid lines show PBR curves, dotted lines show cumulative number of patients with PR/CR up to week 24.
As per definition of PBR, the maximum of the curves is lower than the reported BOR (76.4% vs 60.4% for ruxolitinib and BAT, respectively) because PBR is estimated from the percentage of patients in response at the same point in time, whereas BOR is calculated from the best response, ignoring when this best response occurred and how long it was sustained. Calculating the cumulative number of patients with BOR = CR or PR up to week 24 reaches exactly the BOR rates at week 24 (dashed lines in Fig. 3). However, in contrast to PBR this naive cumulation ignores completely that patients may have lost their response before week 24 (e.g., Pat-ID 6 in Fig. 2) and is shown for comparative purpose only.
The difference between PBR curves with confidence intervals, which provides a more formal comparison than the visual inspection of Fig. 3, clearly shows that superiority of ruxolitinib is achieved within very few weeks after randomization and is maintained over the entire study period (Fig. 4).

Difference in PBR (black line) with 95% CI (blue lines) between ruxolitinib and BAT.
Discussion
Although probability of being in response was considered as a useful method to assess response over time in the statistical literature during the last decades, very few applications can be found in clinical research. In one recent paper, Huang et al. used PBR (referred to as PBIR by Huang et al.) to compare different treatments for renal cell carcinoma [7].
In this post-hoc analysis, we applied PBR to the REACH3 study data to show the benefit of this method when assessing efficacy of cGvHD treatments. PBR provides easily interpretable curves presenting simultaneously the time from treatment start to first response and subsequent failure based on all randomized patients. Results obtained in REACH3 clearly illustrate the superiority of ruxolitinib versus BAT, further confirming the results reported in the original study publication [2]. PBR offers a visual comparison of efficacy over time between treatment arms based on all patients and the entire study period. In contrast, DOR estimates time from first response and visualizes duration of response for the subgroup of patients who responded to treatment only, which can result in a biased assessment of treatment benefit (for example, if a higher percentage of patients reaches the response state in the experimental than in the control arm).
The multistate model and the resulting estimated PBR function considered in this paper were defined in alignment with the definition of efficacy endpoints as pre-specified in the REACH3 study protocol. The design of this multistate model (PBR function), allowing transition from state 0 = not in response to state 1 = in response but NOT state 1 to state 0, as well as the definition of events for the end of response are based on exactly the same criteria as REACH3 efficacy endpoints.
In future work or for other studies, one could extend the model, or alternatively define events differently than done here for REACH3. In particular, as determined in the study protocol, patients were counted as responders only if the first response occurred up to week 24. However, first response to treatment may occur after week 24, i.e., patients who did not respond up to week 24 do not necessarily need to enter the absorbing state 2 at week 24. Furthermore, loss of response was aligned with the definition of DOR, i.e., once a patient enters state 1 = in response, the patient can either stay in that state until the analysis cut-off date or can lose the “in response” status by entering the absorbing state 2, thus ending the duration of response. However, in diseases such as cGvHD, it may also be meaningful to extend the model by allowing transitions from “in response” (state 1) back to “not in response” (state 0) before entering the absorbing state 2. If for instance a patient achieves an overall response of PR by improvement of cGvHD symptoms in several organs at week 8, but subsequently one organ worsened at week 12 (with response maintained in the other organs) and improved again at week 16 without having changed systematic cGvHD treatment, it would be reasonable to assign state 0 = not in response, state 1 = in response, state 0 = not in response and state 1 = in response at study start, week 8, week 12 and week 16, respectively. PBR could be applied to such model extensions.
One of the reasons why applications of PBR can hardly be found in the clinical literature may be the lack of statistical software to perform these analyses. Recently, Xiadong et al. provided the R-package PBIR which can be easily applied within the open-source software R [8]. Due to the special situation that cGvHD first response to treatment in REACH3 was counted up to week 24, we have generated our own R-codes and used PBIR R-package for validation purposes only (PBIR would have cut the curves at week 24).
It would also be useful to have a formal statistical test for comparing the treatments with respect to PBR. We do not elaborate on this topic here for two reasons. Firstly, the difference of PBR curves including pointwise 95% confidence intervals (Fig. 4) allows a good visual comparison between treatment arms, and provides sufficient evidence that the difference between the curves is statistically significant. Secondly, to our knowledge, a statistical test providing a direct generalization of the usual log-rank test is not yet available for the situation described in this paper; its development is subject of forthcoming work. Considering a parametric estimation of PBR curves using the exponential distribution, Ellis et al. proposed a statistical test by comparing the area under the PBR curves (referred to as expected duration of response, EDoR) between treatment arms [5]. Other alternatives (such as a log-rank test of time in response from entering the response state until leaving it for the absorbing state, potentially setting time in response to 0 for those patients who went from state 0 straight to state 2) are conceivable, but a thorough discussion of their properties, interpretational restrictions and precise relation with the PBR curve is beyond the scope of this paper.
As illustrated with the data of REACH3 we strongly believe that PBR can serve as a meaningful efficacy endpoint for the assessment of cGvHD treatments, in addition to ORR/BOR and failure-free survival (FFS) which are recommended as endpoints for clinical trials by the NIH clinical design working group [9]. Compared to these established endpoints PBR provides a more comprehensive summary of treatment efficacy because it integrates several aspects of the treatment benefit (time-to-response, duration of response) into a single measure. Whereas time is not taken into account for ORR/BOR, FFS describes the time to treatment failure only but does neither assess if patients respond to treatment nor the time to response. Further clinical input would be required to include PBR into an updated cGvHD response guideline, also to ensure that consistent criteria are applied across future clinical trials. For example, a clear definition of response duration and end of response would be required. The current guidelines postulate to ‘document durability of response and to determine whether continued treatment is needed to maintain response’ and state that ‘Efforts to document the durability of response are strongly encouraged’, but do not provide clear definitions of response durability [1, 9]. Finally, PBR represents a useful endpoint measure which could be applied for all diseases and indications, for which clinical benefit is assessed by response to treatment in the context of time, demonstrating further utility outside of the cGvHD treatment landscape.
Data availability
Individual data sharing to third parties will not be possible. Access to aggregated data might be granted following review. Such requests can be submitted to the corresponding author for consideration.
References
Lee SJ, Wolff D, Kitko C, Koreth J, Inamoto Y, Jagasia M, et al. Measuring therapeutic response in chronic graft-versus-host disease. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: IV. The 2014 Response Criteria Working Group report. Biol Blood Marrow Transpl. 2015;21:984–99.
Zeiser R, Polverelli N, Ram R, Hashmi SK, Chakraverty R, Middeke JM, et al. Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease. N. Engl J Med. 2021;385:228–38.
Temkin NR. An analysis for transient states with application to tumor shrinkage. Biometrics. 1978;34:571–80.
Begg CB, Larson M. A study of the use of the probability-of-being-in-response function as a summary of tumor response data. Biometrics. 1982;38:59–66.
Ellis S, Carroll KJ, Pemberton K. Analysis of duration of response in oncology trials. Contemp Clin Trials. 2008;29:456–65.
Tsai WY, Luo X, Crowley J. The probability of being in response function and its applications. In: Matsui S, Crowley J, eds. Frontiers of biostatistical methods and applications in clinical oncology. Singapore: Springer Singapore; 2017. p. 151–64.
Huang B, Tian L, McCaw ZR, Luo X, Talukder E, Rothenberg M, et al. Analysis of response data for assessing treatment effects in comparative clinical studies. Ann Intern Med. 2020;173:368–74.
Xiaodong L, Huang B, Tian L. PBIR: estimating the probability of being in response and related outcomes. R package version 0.1-0 (2020) 2020. Available from: https://CRAN.R-project.org/package=PBIR
Martin PJ, Lee SJ, Przepiorka D, Horowitz MM, Koreth J, Vogelsang GB, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: VI. The 2014 Clinical Trial Design Working Group Report. Biol Blood Marrow Transpl. 2015;21:1343–59.
Acknowledgements
This study was sponsored by Novartis Pharma AG. The authors would like to thank the patients, their families and investigators and staff at participating study sites. We are also grateful to one reviewer whose comments motivated the generation of Supplementary Material S2. Editorial assistance was provided by Soracha Ward, PhD of Novartis Ireland, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). These data were presented in part at the American Society of Hematology Congress, New Orleans, 10–13 December 2022. These data are reproduced in part from Hollaender N, Glimm E, Gauvin J, Stefanelli T, and Zeiser R. The Probability of Being in Response (PBR): A Novel Efficacy Endpoint for Chronic Graft Versus Host Disease (GvHD) Applied to the Reach-3 Study of Ruxolitinib Versus BAT, Blood (2022) 140 (supplement 1): 10521–10522 with permission from Elsevier.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the conception and design or analysis and interpretation of the data, and the drafting and critical review of the manuscript. All authors approved the final version of the manuscript for publication.
Corresponding author
Ethics declarations
Competing interests
NH and TS are current employees of Novartis. EG and JG hold equity in and are current employees of Novartis. RZ received honoraria from and is on the speaker’s bureau for Incyte, Mallinckrodt, and Novartis, and has consulted for Incyte and Novartis.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hollaender, N., Glimm, E., Gauvin, J. et al. A novel approach to visualize clinical benefit of therapies for chronic graft versus host disease (cGvHD): the probability of being in response (PBR) applied to the REACH3 study. Bone Marrow Transplant 59, 12–16 (2024). https://doi.org/10.1038/s41409-023-02128-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41409-023-02128-8
