
Abstract
Purpose
To evaluate intravitreal conbercept injection for treatment of macular oedema secondary to central retinal vein occlusion (CRVO) in Chinese patients during 1-year follow-up in the real-world setting.
Methods
Twenty-seven eyes of 27 patients with macular oedema associated with CRVO were retrospectively reviewed. The eyes received monthly intravitreal conbercept injection (0.5 mg in 50 µl) for 3 months. From then on, the patients were followed up every month and received injection pro re nata (PRN) up to 12 months. The primary outcome measurements included changes of best-corrected visual acuity (BCVA) and central retinal thickness (CRT) from baseline to month 3 and month 12. Other outcome measurements included proportion of patients gaining ≥15 letters in BCVA at month 3 and 12, the mean number of injections and safety concerns.
Results
The mean BCVA gain from baseline was 12.7 ± 7.6 letters at month 3 and 14.8 ± 9.6 letters at month 12. The mean CRT reduction from baseline was 374.5 ± 280.7 μm at month 3 and 428.2 ± 241.3 μm at month 12. The proportion of patients who gained ≥15 letters in BCVA was 45.1% at month 3 and 52.9% at month 12. The mean number of injections was 7.6 ± 1.5. No severe local and systemic complications occurred following injection.
Conclusions
Intravitreal conbercept injection by three monthly loading doses followed by PRN treatment regimen was safe and efficacious for patients with macular oedema secondary to CRVO through 1-year follow-up.
Similar content being viewed by others

Introduction
Central retinal vein occlusion (CRVO) is a common retinal vascular disorder that can result in severe visual acuity loss. The prevalence of RVOs is about 0.5% in the 2008 general world population and is estimated to affect more than 16 million people worldwide [1, 2]. In China, the 10-year incidence rate of RVO for those 40 years of age or older at baseline is 1.9 per 100 and is estimated to affect 3.2 million people [3, 4]. Macular oedema (MO) is a frequent cause of visual impairment in CRVO. Studies show that increased production of vascular endothelial growth factor (VEGF) occurring early in RVO is a major contributor to the evolution and persistence of MO and haemorrhages [5]. Therefore, nowadays, anti-VEGFs have become the standard of care for treating CRVO-associated MO. Three major anti-VEGF medications including intravitreal ranibizumab (Lucentis; Genentech, Inc. and Novartis International AG, Basel, Switzerland), aflibercept (Eylea; Regeneron, Tarrytown, NY and VEGF-Trap Eye;Bayer AG, Leverkusen, Germany) and bevacizumab (Avastin; Genentech, South San Francisco, CA) have showed marked visual benefit in CRVO in numerous studies [6,7,8].
Conbercept (Lumitin; Chengdu Kang Hong Biotech Co, Ltd, Sichuan, China) is a fusion protein composed of the extracellular domain 2 of VEGF receptor 1 and 1 extracellular domains 3 and 4 of VEGF receptor 2 combined with the Fc portion of the human immunoglobulin G1. In preclinical trials, the binding affinity of conbercept for VEGF is substantially greater than that of bevacizumab, ranibizumab, or aflibercept [9,10,11]. Like aflibercept, it also shows a very high affinity for placental growth factor, which can act as a mitogenic, chemotactic and vascular permeability factor for endothelial cells. Phases II and III clinical trials have demonstrated good efficacy on MO resolution and acceptable safety, when administered intravitreally for up to 12 months in patients with neovascular age-related macular degeneration [12, 13]. Recently, efficacy and safety of conbercept in treatment of MO secondary to RVO have been reported by FALCON study [14]. In this prospective, Phase II clinical trial, 30 branch RVO patients and 30 CRVO patients received intravitreal injections of conbercept (IVC) monthly up to 3 months, followed by monthly evaluation and injection pro re nata (PRN) to month 9. The result of the study demonstrated a generally favourable safety and tolerability profile, as well as efficacy in the treatment of MO due to RVO. However, the report of treatment of MO associated with CRVO with IVC in the real-life setting with long-time follow-up is lacking. Therefore, the purpose of the study was to assess the safety and efficacy of IVC in the treatment of MO in the Chinese patients with CRVO in the period of 12-month follow-up. Our findings supported the result of FALCON study, even with ischaemic cases included.
Subjects and methods
Patients
Twenty-seven eyes of 27 Chinese patients with MO associated with CRVO from September of 2016 to January of 2018 were consecutively included and retrospectively reviewed. The inclusive criteria were as follows: best-corrected visual acuity (BCVA) was ≤73 Early Treatment Diabetic Retinopathy Study letters (0.5 decimal equivalent) without lowest limit and the central retina thickness (CRT) was ≧300 μm measured by spectral-domain optical coherence tomography (SD-OCT; Spectralis; Heidelberg Engineering, Heidelberg, Germany). The patients with MO secondary to causes other than CRVO or lack of adequate follow-up information were excluded. The studied eyes had no prior ocular surgery, trauma or laser history, as well as abnormal ocular conditions including diabetic retinopathy, glaucoma and ocular inflammation. All patients were treatment naive. Eyes with a relative afferent pupillary defect (RAPD) or/and total area of retinal ischeamia ≧10 disc area (DA) defined by fundus fluorescent angiography (FFA) were also included in this study. The study was approved by the local ethical committee in Beijing Tongren Hospital and adhered to the tenets of the Declaration of Helsinki. Off-label use of the drug and its potential risks and benefits were discussed extensively with all patients. All of them provided the written informed consent before the injections.
The patients were examined BCVA using international decimal vision chart (converting into EDTRS letters according to the prior publication [15]), intraocular pressure (IOP) via pneumotomometer (Topcon, Tokyo, Japan), biomicroscopy of the fundus and anterior segment, SD-OCT before procedure. FFA was done before or after intravitreal injection when retinal haemorrhage was mostly resolved.
Treatment
The IVC (0.5 mg/0.05 mL) were given monthly in the loading phase of 3 months. During month 3 through month 12, patients were evaluated monthly and received injections as needed or PRN (so called 3+PRN). Patients received re-treatment in the following circumstances: (1) The increase of ≧50 μm in CRT compared with the lowest previous measurement. (2) The loss of ≧5 EDTRS letters compared with the previous measurement. (3) The presence of new or persistent cystic retinal changes, sub-retinal fluid, or neuroepithelial detachment. (4) The presence of new macular haemorrhage or retinal neovascularization. (5) At the investigator’s discretion. If ≧1 re-treatment criterion was met, eyes received an injection. Pan-retinal photocoagulation (PRP) was performed on the patients with extensive retinal non-perfusion area (≧30 DA).
Outcome measurements
The primary out outcome measures included changes in BCVA and CRT from baseline to month 3 and 12. Additional outcome measurements included proportion of patients gaining ≧15 letters in BCVA at month 3 and 12 from baseline, the mean number of injections and complication after injection.
Statistics
All statistical analyses were performed with SPSS 19.0 statistics (IBM SPSS Statistics for Windows, NY, USA). The changes in BCVA and CRT between baseline and follow-up were evaluated by pair t-test at a two-side significance level of 5%. There was no selection bias and all patients treated and followed up as required during the study period were included in the analysis.
Results
Patients demographics and baseline characteristics
Twenty-seven eyes of 27 patients were included in the study. The baseline characteristics were summarized in Table 1.
Treatment outcome
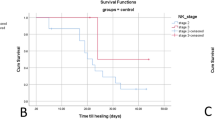
The mean baseline BCVA was 45.1 ± 11.0 letters before injections. It significantly increased to 57.8 ± 14.7 letters at month 3, with the mean gain of 12.7 ± 7.6 letters (t = 7.59, P < 0.001). At month 12, it improved to 59.9 ± 12.6 letters with mean gain of 14.8 ± 9.5 letters (t = 7.71, P < 0.001). The changes in the BCVA are shown in Fig. 1a. In total, 45.1% and 52.9% of the patients gained ≧ 15 letters from baseline at month 3 and 12, respectively. BCVA in no eyes dropped from baseline to month 3. At month 12, none of the 27 patients lost ≧ 15 letters and BCVA in 89.2% (24/27) of the patients had improved from the baseline. On the other hand, the mean baseline CRT was 707.0 ± 252.3 μm. It was dramatically decreased to 312.5 ± 80.3 μm at month 3 with mean reduction of 374.5 ± 280.7 μm (t = 7.71, P < 0.001). At month 12, it continued to reduce to 278.8 ± 68.8 μm with mean reduction of 428.2 ± 241.3 μm (t = 7.60, P < 0.001). The changes in the CRT are shown in Fig. 1b. The results showed that one half of the patients reduced to normal thickness following three injections. It was noted that there was a marked increase in CRT at month 4 when the treatment switched to PRN phase, which corresponded with the decrease in BCVA. From month 5, the trend of decrease in CRT and improvement in BCVA was recovered and maintained to month 12 by using PRN dosing regimen.

The mean changes of best correct visual acuity (a) and central retinal thickness (b) from baseline over 12 months were shown. *P < 0.001 compared with baseline.
Seven patients with BCVA ≦ 35 letters (0.1 decimal equivalent) also achieved visual and anatomic improvement after treatment. Three patients received PRP due to extensive retinal ischaemia. No patients with non-ischaemic CRVO progressed to ischaemic retinopathy or ischaemic CRVO developed to ocular neovascularization. The mean number of injections at 12-month follow-up was 7.6 ± 1.5 (5–10 injections)
No severe drug-related ocular or systemic adverse events (AE) were observed. Mild AE included conjunctival haemorrhage, vitreous opacity and temporarily elevated IOP.
Figure 2 described the case of 63-year-old man with MO secondary to CRVO, who was successfully treated using 3+PRN intravitreal conbercept injection.

The 63-year-old man had a vision loss for 3 months with BCVA as 0.05 and central retinal thickness (CRT) up to 669 μm on OCT (a). The BCVA improved to 0.5 and CRT reduced to 252 μm following 3 months loading dose of injection (b). The CMO recurred at month 4 when switched to PRN treatment with increase of CRT to 338 μm and slight drop of BCVA to 0.4 correspondently (c). After retreatment, the cysts were resolved at month 5 and BCVA resumed to 0.5 (d). He received another 3 injections PRN and the vision increased to 0.7 with well-maintained macular anatomy at month 12 (e).
Discussion
Our present study showed that treatment of MO secondary to CRVO in Chinese patients with IVC achieved significant improvement in visual acuity and macular anatomy at both month 3 and month 12. The BCVA were rapidly increased after first three monthly loading doses with 12.7 letters gain from the baseline and continued to improve during the maintenance period with 14.2 letters gain at month 12. Correspondingly, the CRT were dramatically decreased at month 3 with mean reduction of 312.5 μm, and maintained during next 9 months with mean reduction of 428 μm at the end of follow-up. In total, 45.1% and 52.9% of the patients produced more than 15 letters gain from the baseline at month 3 and month 12, respectively. No severe ocular and systemic AE reported in the present study. Taking together, the data from our real-world practice indicated efficacy and safety of IVC in treatment of Chinese patients with MO associated with CRVO in the long-term follow-up period.
Anti-VEGFs have become the first-line therapy for CRVO. There are two types of anti-VEGF medications. Ranibizumab and bevacizumab belong to humanized monoclonal immune-globlin-G1 antibody that binds to all isoforms of VEGF-A while aflibercept and conbercept belong to recombinant fusion protein consisting of VEGF extracellular-binding domains [9, 16,17,18]. In addition to competitive inhibition of all kinds of VEGF, recombinant fusion protein also binds placental growth factors 1 and 2, which suggests more extensive and powerful effect compared with monoclonal antibody. Three randomized clinical trials (RCT) demonstrated the efficacy of the anti-VEGFs as the primary treatment modality in patents with MO secondary to CRVO, CRUISE for Ranibizumab [6], as well as COPERNICUS [7] and GALILEO [19] for aflibercept. The treatment regimen used was initial loading dose of six monthly injections followed by PRN protocol (6+PRN). Despite the availability of these treatment guidelines, the optimal protocol regarding choice of anti-VEGF reagents and dosing regimen has been in dispute. Recently, Hykin et al. reported the outcome of the LEAVO Study [20], which demonstrated in the CRVO-related MO, aflibercept treatment was noninferior to ranibizumab treatment at 100 weeks and the bevacizumab was not noninferior compared with ranibizumab and aflibercept. In addition, fewer injections were required for aflibercept compared with ranibizumab, suggesting a potential advantage to use of recombinant fusion protein in similar population. Conbercept, which is largely similar to aflibercept in molecular structure but demonstrated greater binding affinity for VEGF due to adding domain 4 from VEGFR 2, was used with 3+PRN regimen in our study to treat patients with MO associated with CRVO. The trend of visual and anatomic achievement was quite similar to above-mentioned RCT studies indicating rapid and significant increase of BCVA and reduction of CRT in the loading dose phase of injection and maintained quite well in the PRN dosing phase. At month 12, the mean gain of BCVA (14.8 letters) using IVC in our study was similar or even little more than intravitreal injection of ranibizumab (13.9 letters) in the CRUISE study, but was less than intravitreal injection of aflibercept in the COPERNICUS (16.2 letters) and GALILEO (16.9 letters) study, suggesting the possibility of better effect of recombinant fusion protein than monoclonal antibody, but may need more initial fixed loading dose of injections if better VA gain wanted. As we expected, the mean number of injections in the 12-month follow-up period in the present study was 7.6, which was less than the three RCT studies with initial six monthly loading doses (8.5–8.7 injections). On the other hand, the outcomes of the LEAVO study supported our findings but provided more flexible monitoring schedule (four initial loading injections and extension of visit interval from 4 to 8 weeks, if the retreatment criteria have not been met at three consecutive visits) to reduce the monthly follow-up burden.
Falcon study was an open-label, non-controlled, 9-month trials assessing the efficacy and safety of IVC in the MO secondary to RVO by 3+PRN dosing regimen. The results showed that the mean gain of BCVA was 11.5 letters and 14.2 letters while the mean reduction of CRT was 380.5 μm and 420.5 μm from the baseline at month 3 and month 9, respectively. It was noted that ischaemic RVO patients with RAPD positive were not included in the study and the occlusion in all patients occurred within 6 months. In contrast, our retrospective study included three patients with ischaemic CRVO, enrolled the patients with longer duration of disease (up to 10 months) and took longer follow-up period, which was more representative of real-world setting. However, similar or even better visual and anatomical outcome seemed to be achieved compared with the trial at each time point up to month 9. Some of the non-ischaemic patients with poor vision (BCVA < 35 letters) as well as excessive retinal thickness (>1000 μl) also achieved three lines BCVA gain given that ellipsoid zone was intact as shown in the case report. In addition, the VA of all three ischaemic CRVO patients was not dropped following receiving the regular treatment, suggesting all types of patients might benefit from the IVC in the 1-year follow-up. As Falcon, our study also indicated a fluctuation in terms of VA gain and CRT reduction at month 4 when switch of treatment to PRN dosing, but resumed rapidly with re-treatment, stressing the importance of close follow-up and re-treatment as needed. Besides, the number of injections did not seem to increase with prolonged observation period in our present study by showing 7.6 injections in 12-month versus 7.59 injections in 9 month in Falcon.
Our study showed no patients with non-ischaemic CRVO progressed to ischaemic retinopathy or ischaemic CRVO developed to ocular neovascularization. PRP was performed on the patients with extensive non-perfusion area to reduce the risk of development to neovascularization. Whether scatter photocoagulation promotes resolution of MO, reduces the need for VEGF antagonists, and improves outcomes in patients with RVO has been in dispute. Recently, the result of RELATE study demonstrates that laser to non-perfused area does not improve visual outcomes or reduce the number of anti-VEGF injections in the RVO patients [21].
No severe ocular and systemic AEs occurred except some common and minor AEs reported in other studies. The limitation of present study included nature of retrospective analysis, comparably small number of cases and lack of control group. Larger case numbers, control groups with blank or other popular anti-VEGF agents may be used to further confirm the conclusion or indicate the difference between conbercept and other type of anti-VEGFs in the management of CRVO.
In conclusion, our real-world data demonstrated efficacy and safety of IVC in the treatment of MO resulting from a variety of CRVO in the Chinese patients in the 12-month follow-up period. Three fixed monthly IVC followed by PRN treatment was an efficacious treatment strategy for visual and anatomic achievement. More initial fixed injections may get a better VA gain in the long-term outcome result.
Summary
What was known before
Anti-VEGFs have become the first-line therapy for retinal vein occlusion.
Conbercept is a recently developed anti-VEGF reagent that belongs to fusion protein family consisting of VEGF extracellular-binding domains. Efficacy and safety of conbercept in treatment of MO secondary to RVO have been reported by a Phase II clinical trial with 9-month follow-up.
What this study adds
We evaluated intravitreal conbercept injection for treatment of macular oedema secondary to central retinal vein occlusion in Chinese patients during 1-year follow-up in real-world setting.
References
Rogers S, McIntosh RL, Cheung N, Lim L, Wang JJ, Mitchell P, et al. International Eye Disease Consortium. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010;117:313–9.
Jaulim A, Ahmed B, Khanam T, Chatziralli IP. Branch retinal vein occlusion: epidemiology, pathogenesis, risk factors, clinical features, diagnosis, and complications: an update of the literature. Retina. 2013;33:901–10.
Yen YC, Weng SF, Chen HA, Lin YS. Risk of retinal vein occlusion in patients with systemic lupus erythematosus: a population-based cohort study. Br J Ophthalmol. 2013;97:1192–6.
Zhou JQ, Xu L, Wang S, Wang YX, You QS, Tu Y, et al. The 10-year incidence and risk factors of retinal vein occlusion. Ophthalmology. 2013;120:803–8.
Campochiaro PA, Hafiz G, Shah SM, Nguyen QD, Ying H, Do DV, et al. Ranibizumab for macular edema due to retinal vein occlusions: implication of VEGF as a critical stimulator. Mol Ther. 2008;16:791–9.
Campochiaro PA, Brown DM, Awh CC, Lee SY, Gray S, Saroj N, et al. Sustained benefits from ranibizumab for macular edema following central retinal vein occlusion: twelve-month outcomes of a phase III study. Ophthalmology. 2011;118:2041–9.
Heier JS, Clark WL, Boyer DS, Brown DM, Vitti R, Berliner AJ, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion: two-year results from the COPERNICUS study. Ophthalmology. 2014;121:1414–20.
Prager F, Michels S, Kriechbaum K, Georgopoulos M, Funk M, Geitzenauer W, et al. Intravitreal bevacizumab (Avastin) for macular oedema secondary to retinal vein occlusion: 12-month results of a prospective clinical trial. Br J Ophthalmol. 2009;93:452–6.
Wang Q, Li T, Wu Z, Wu Q, Ke X, Luo D, et al. Novel VEGF decoy receptor fusion protein conbercept targeting multiple VEGF isoforms provide remarkable anti-angiogenesis effect in vivo. PLoS One. 2013;8:e70544.
Zhang M, Yu D, Yang C, Xia Q, Li W, Liu B, et al. The pharmacology study of a new recombinant human VEGF receptor-fc fusion protein on experimental choroidal neovascularization. Pharm Res 2009;26:204–10.
Yu DC, Lee JS, Yoo JY, Shin H, Deng H, Wei Y, et al. Soluble vascular endothelial growth factor decoy receptor FP3 exerts potent antiangiogenic effects. Mol Ther. 2012;20:938–47.
Li X, Xu G, Wang Y, Xu X, Liu X, Tang S, et al. Safety and efficacy of conbercept in neovascular age-related macular degeneration: results from a 12-month randomized phase 2 study: AURORA study. Ophthalmology. 2014;121:1740–7.
Liu K, Song Y, Xu G, Ye J, Wu Z, Liu X, et al. PHOENIX Study Group. Conbercept for treatment of neovascular age-related macular degeneration: results of the Randomized Phase 3 PHOENIX Study. Am J Ophthalmol. 2019;197:156–67.
Sun Z, Zhou H, Lin B, Jiao X, Luo Y, Zhang F, et al. Efficacy and safety of intravitreal conbercept injections in macular edema secondary to retinal vein occlusion. Retina. 2017;37:1723–30.
Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing snellen visual acuity measurements. Retina. 2010;30:1046–50.
Ferrara N, Damico L, Lowman H, Kim R. Development of ranibizumab, an anti-vascular endothelial growth factor antigen binding fragment, as therapy for neovascular age-related macular degeneration. Retina. 2006;26:859–70.
Ferrara N, Hillan KJ, Gerber HP, Novotny W. Discovery and development of bevacizumab, an anti-VEGF antibody for treating cancer. Nat Rev Drug Discov. 2004;3:391–400.
Holash J, Davis S, Papadopoulos N, Croll SD, Ho L, Russell M, et al. VEGF-trap: a VEGF blocker with potent antitumor effects. Proc Natl Acad Sci USA. 2002;99:11393–8.
Korobelnik JF, Holz FG, Roider J, Ogura Y, Simader C, Schmidt-Erfurth U, et al. GALILEO Study Group. Intravitreal aflibercept injection for macular edema resulting from central retinal vein occlusion: one-year results of the Phase 3 GALILEO Study. Ophthalmology. 2014;121:202–8.
Hykin P, Prevost AT, Vasconcelos JC, Murphy C, Kelly J, Ramu J, et al. LEAVO Study Group. Clinical effectiveness of intravitreal therapy with ranibizumab vs aflibercept vs bevacizumab for macular edema secondary to central retinal vein occlusion: a randomized clinical trial. JAMA Ophthalmol. 2019;29. https://doi.org/10.1001/jamaophthalmol.2019.3305.
Campochiaro P, Hafiz G, Mir TA, Scott AW, Solomon S, Zimmer-Galler I, et al. Scatter photocoagulation does not reduce macular edema or treatment burden in patients with retinal vein occlusion: the RELATE trial. Ophthalmology. 2015:122:1426–37.
Funding
This work was supported by Beijing Municipal Health System High-level Professionals training Program 2015 and Key research programme of Beijing Institute of Ophthalmology 2019.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zeng, Hy., Liu, Q., Li, Xx. et al. One-year efficacy of intravitreal conbercept injection for macular oedema secondary to central retinal vein occlusion in Chinese patients. Eye 34, 1459–1464 (2020). https://doi.org/10.1038/s41433-020-0827-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-020-0827-y
