
Abstract
Apical periodontitis (AP) is a condition characterized by inflammatory and infectious components in the tooth canal. AP affects periradicular tissues and has systemic repercussions. Physical exercise is a structured activity that requires cardiorespiratory function, and can modulate the inflammatory profile in pathological conditions. As a result, this study aimed to determine the effects of aerobic physical training (PT) on the alveolar bone with and without AP, and its systemic inflammatory repercussions. AP was induced in the mandibular first molars, and PT was performed on a treadmill for five consecutive days over four weeks, with progressive increases in speed and activity time. Blood samples were collected to determine serum cytokine levels using immunoassays, and alveolar bone samples were collected for histopathological evaluation, lesion volume and microarchitecture assessment using computed microtomography. Animals with AP had increased pro-inflammatory cytokines levels compared to those without AP; however, these levels were attenuated or restored by PT. Compared to the AP group, the AP + PT group had a smaller lesion volume and greater preservation of the bone trabeculae in the remaining alveolar bone surrounding the lesion. In overall, PT minimized the severity of AP proving to be a valid strategy for individuals undergoing endodontic treatment.
Similar content being viewed by others


Introduction
Physical activity is defined as any skeletal movement that requires more energy than that used by the body at rest1. Physical training differs from physical activity in terms of planning and structure, and considers the duration, frequency, and intensity of the activity2. Physical exercise promotes overall health by preventing and reducing inflammatory processes associated with various diseases3. Accordingly, several training modalities can stimulate biological systems, such as the musculoskeletal and cardiorespiratory systems, and different planning strategies are required to achieve the beneficial effects of physical exercise. Thus, to be considered a successful exercise program, moderate-intensity training should be recommended, as people inexperienced in high-intensity exercise may discontinue this activity. High-intensity training can also increase the risk of injury or acute cardiovascular events4.
The effects of physical training may be related to its involvement in inflammatory and immunological mechanisms5. Physical training modulates cytokines produced and released by the skeletal muscles, known as myokines, such as interleukin-6 and interleukin-86. As a result, physical training has been proposed as a non-pharmacological strategy to reduce systemic inflammation5. A systematic review concluded that interleukin-6, tumor necrosis factor-α, interferon-γ, and C-reactive protein are key biomarkers of reduced inflammation caused by physical exercise in patients with atherosclerosis, a progressive and prevalent inflammatory disease7.
Apical periodontitis (AP) is another highly prevalent disease that causes an inflammatory reaction in the periapical tissues due to microbial infection in the dental pulp8. Infection occurs in the root canal after the pulp becomes necrotic due to caries, trauma, periodontal disease, or iatrogenesis, or when the pulp is absent due to previous root canal treatment. Once the infection is established in the root canal, it progresses in the apical direction, eventually reaching the periradicular tissues through the apical and lateral foramina, and promotes inflammation. AP is diagnosed, and depending on different bacterial- and host-related factors, this disease can be symptomatic (acute) or asymptomatic (chronic)9. AP advancement can promote serious alterations in the dental supporting apparatus as it progressively causes bone resorption, which can even culminate in tooth loss10. This severe pathogenic mechanism profile has significant implications in terms of aggression, as it is intrinsically related to systemic manifestations, such as the modulation of blood inflammatory markers11.
The levels of interleukin, C-reactive protein, and immunoglobulin are indicators of low-grade systemic inflammation caused by AP11. Cytokines participate in the degradation of extracellular matrix constituents and promote changes in periodontal cells. The exit of bacteria and their products from the apical foramen into periapical tissues triggers proinflammatory and anti-inflammatory mediators, including cytokines and other enzymes responsible for the activation of the inflammatory response. When the levels of inflammatory mediators reach a certain threshold, bone resorption pathways are activated, stimulating the action of fibroblasts and osteoblasts, which promote bone resorption12.
Endodontic infections can significantly influence the development and maintenance of systemic disorders, either through hematogenous dissemination of the microorganisms themselves, dissemination of their toxins, or induction of a low-intensity systemic inflammatory response11. Based on the benefits of physical training in modulating systemic features, this study aimed to determine the effects of physical training on rats with AP through an evaluation of both local and systemic repercussions.
Results
Evaluation of the systemic cytokine concentrations (IL-1β, TNF-α, IL-6, IL-10)
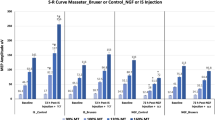
Plasma levels of TNF-α (Fig. 1B) and IL-6 (Fig. 1C) were increased in the AP group compared to the control (adj. p value: 0.0063) and training (adj. p value: 0.0055) groups. When the animals with AP were subjected to physical training, the TNF-α concentration was reduced to values equivalent to those of the control (adj. p value: 0.777). Overall, AP increased the level of IL-6, which was significantly attenuated by physical training (adj. p = 0.0230). The levels of IL-1β and IL-10 did not change in any of the experimental groups.

Plasma cytokine concentrations of physically trained animals with apical periodontitis. Plasma concentration of IL-1beta (A), TNF-alpha (B), IL-6 (C), and IL-10 (D). The results are expressed as pg/mL. Different letters indicate statistically significant difference (p < 0.05). The analysis was performed using one-way ANOVA with Tukey’s post hoc test (n = 8/per group).
Physical training modulates the inflammatory response and minimizes the damages to the remaining alveolar bone
When the physically trained group with AP (G,H) was compared to the group with AP only (E,F), the interradicular bone was found to be more preserved in the furcation region of the physically trained group with AP,). Similar to the apical region, greater bone damage was identified in the group with AP (F) as the lesion area in this group was more extensive than that in the physically trained group with AP (H), which showed better preservation of the alveolar bone (Fig. 2), ultimately complementing and confirming the micro-CT results.

Implication of moderate-intensity physical training on inflammatory modulation in the furcation and apical regions of animals with apical periodontitis. 40 × magnification of the furcation and apical regions, respectively, of the maxillary first molar in the control (A, B), physical training (C, D), apical periodontitis only (E, F), and physically training + apical periodontitis (G, H) groups. Scale bar = 100 μm. In A, C, E, and D, the cross ( +) represents interradicular bone. In B and D, the star (✰) represents the periodontal ligament space. In F and H, the asterisk (*) represents the lesion area.
Physical exercise minimizes bone damage in rats with AP
The osteomodulatory effects of physical training on the remaining alveolar bone in rats with AP are shown in Fig. 3. Although no changes in trabecular thickness were observed beyond the expected thickness in the AP groups (p < 0.05; Fig. 3A), physical training could attenuate the impairment caused by AP over trabecular separation (adj. p value: < 0.0001; Fig. 3B).

Effects of physical training on the alveolar bone of animals with apical periodontitis. Trabecular thickness in millimeters (A). Trabecular separation in millimeters (B). Trabecular number in 1/millimeters (C). Bone volume per tissue volume in percentage (D). The results are expressed as mean ± SEM. Different letters indicate a statistically significant difference (p < 0.05). The analysis was conducted using one-way ANOVA with Tukey’s post hoc test (n = 8/group).
The trabecular number did not change in any of the experimental groups (Fig. 3C); however, the proportions of bone volume and tissue volume were significantly attenuated by physical training in animals with AP (adjusted p value: 0.0042; Fig. 3D).
Physical training reduces the volume of induced periapical lesion in rats
Regarding apical periodontitis damage, the microtromographic assessment revealed a significant increase in lesion volume in sedentary animals compared to control and trained animals (Fig. 4; adj. p-value: < 0.0001). However, physical training attenuated the lesion volume compared to that found in lesioned and sedentary animals (adjusted p-value: 0.0029).

Effects of physical training on the lesion volume of animals with apical periodontitis. Representative sagittal and transverse slices of the hemimandibles of animals in the control (A, B, respectively), physical training (C, D, respectively), apical periodontitis (E, F, respectively), and apical periodontitis + physical training (G, H, respectively) groups. The blue dashed lines on the sagittal images represent the volume of interest used to measure lesion volume (mm3), and the blue dashed lines on the transverse images represent the region of interest for evaluating the quality of the remaining alveolar bone. Different letters indicate a statistically significant difference (p < 0.05). The analysis was performed using one-way ANOVA with Tukey’s post hoc test (n = 8/group).
Discussion
To the best of our knowledge, this is the first study to demonstrate that physical training comprising structured frequency and speed reduces the systemic inflammatory profile triggered by AP and attenuates the morphological damage to the alveolar bone of rats, including bone quality and periapical lesion area. This preclinical study provides important scientific data that are relevant in endodontics and sports dentistry, and highlights the beneficial effects of physical training in the minimization of AP-induced damage.
Different protocols are available for inducing AP in experimental models13,14,15,16,17,18. In this study, AP was induced by accessing the pulp chamber and exposing it to the oral environment, enabling infection and inflammation. This model has been well established in previous studies14,15,19. A 28-day experimental period is employed because periapical lesions actively expand for 3–4 weeks after pulpal exposure (active phase) and progress slowly thereafter (chronic phase)20.
AP can be either acute or chronic. Acute infections are caused by highly virulent bacteria or the synergistic effects of different species. Acute infections are characterized by a high concentration of bacteria that can invade tissues and reduce host resistance, while chronic AP is usually associated with less-virulent bacterial communities. AP contributes to low-grade systemic inflammation, leading to an overall increase in the levels of systemic inflammatory mediators21. This chronic inflammatory condition is associated with increased inflammatory cell infiltration and serum cytokine levels, which may affect systemic health14. Studies on animals with AP revealed an increase in the blood levels of TNF-α, IL-1β, IL-2, IL-6, IL-10, MMP-1, MMP-2, C-reactive protein (CRP), and immunoglobulin (IgA, IgG, and IgM)11,14. Thus, therapies and strategies that can minimize the high systemic inflammatory cytokine levels in this condition must be examined to ultimately reduce the predisposition to systemic diseases and progression of the lesion itself.
The cytokine network is a fundamental part of the immune/inflammatory response scenario of AP. In fact, the cytokine network plays an important role along with components of the immune system, vasoactive amines, and metabolites of arachidonic acid10. Plasma cytokine evaluation revealed alterations caused by both AP and physical training (Fig. 1). Animals with AP had higher TNF-α levels than control animals; however, animals with AP that underwent physical training showed a statistically significant decrease in the level of these proinflammatory markers compared to untrained animals with AP. The levels of TNF-α in the AP + PT group were also reduced to levels similar to those found in animals without AP (control or physical training only). TNF-α produces a wide range of effects on different cell types, thereby affecting immune and proinflammatory responses22. TNF-α and interleukins are involved in periapical pathogenesis related to bone resorption mechanisms23,24. A study revealed bone extracellular matrix destruction by stimulating the proteolytic activity of plasminogen and activating osteoclasts due to the presence of TNF-α23. The involvement of TNF-α in bone destruction caused by AP may explain the relation between the reduced levels of this cytokine and the minimization of bone destruction after physical activity.
Lesion volume and bone quality were evaluated using micro-CT, a non-destructive method that enables an accurate three-dimensional evaluation of the cortical and trabecular bone25,26. Notably, the alveolar bone microstructure in rats differs from that of other bones owing to its neuroectodermal origin. In fact, the alveolar bone microstructure consists of compact bone with highly mineralized plate-like trabeculae, limited bone marrow, large trabecular thickness, and reduced number of trabeculae and trabecular distances. Changes in these alveolar bone microstructures can be caused by AP, resulting in the resorption of the apical region, which increases the chances of bone destruction13. Based on our findings, animals with AP had alterations in the alveolar bone structure compared to animals without AP. In particular, AP increased the distance between the trabeculae and decreased the trabecular thickness and bone volume (Fig. 3). According to the literature, AP modulates such changes in the alveolar bone of rats mainly due to alterations in bone metabolism caused by cytokines and pathway activation in the blood supply27.
Interestingly, the AP-induced damage to the alveolar bone structure might be reduced by physical activity. The trained animals with AP had a reduced distance between the trabeculae and a higher percentage of bone volume than sedentary animals with AP. Physical training may modulate bone metabolism by attenuating the harmful effects exerted on its microstructure. Furthermore, the lesion volume due to AP was reduced after physical training. Reduced lesion volume is an remarkable finding that can provide suggestions for the modulation of AP pathogenesis by physical training. The smaller dimensions of the lesions in the trained animals are shown in Fig. 4. A smaller lesion can attenuate bone damage and systemic repercussion caused by AP and is associated with a better prognosis28. These volume proportions suggest that the alveolar bone of trained rats has a microarchitecture that is more resistant to lesion progression and may be less affected by the inflammatory immune response.
IL-6 is another cytokine involved in AP. The production of IL-6 occurs after the secretion of TNF-α and IL-1. Thereafter, IL-6 may inhibit the liberation of these cytokines, assuming control over vascular permeability and osteoclast differentiation29. Overproduction of IL-6 has been found to be related to the activity of macrophages and neutrophils present in the first stages of periapical lesion formation29. Prior studies have suggested a correlation between high IL-6 levels and larger lesion volume30. Based on our findings, physical training reduced IL-6 levels in animals with AP. This modulatory effect of physical exercise on IL-6 highlights the magnification repercussions of the lesion volume. The levels of IL-6 may be associated with a different remodeling process, which could explain our micro-Ct findings.
In accordance with the microtomography findings, histopathological analysis revealed greater preservation of the remaining alveolar bone in the AP + PT group than that in the AP group. Periapical lesions are histologically characterized by fibrous and granulated tissues infiltrated by different inflammatory cells31. Histopathological photomicrographs revealed inflammatory infiltrates in the lesion area. An in vivo study comprising a histological analysis revealed that physical exercise had beneficial effects on bone remodeling in diabetic rats32.
Low-grade systemic inflammation promoted by AP leads to an imbalance in the mechanisms involved in the modulation of serum cytokine levels, mainly related to a decrease in the activity of regulatory T lymphocytes (Tregs)24. Tregs are a subpopulation of T-cells responsible for suppressing T-cell responses and limiting disease progression. In human periodontitis, Tregs can express TNF- α, which might regulate the immunologic process of periodontitis. IL-6 negatively regulates T cell differentiation, the inflammatory response, and osteoclast differentiation33. Thus, the role of physical activity and exercise modulation in cytokine imbalance may be related to periodontitis and a reduction in periapical lesion progression34.
The effects of physical training on bone tissue have garnered attention in studies related to sports and systemic diseases with bone implications, such as osteoporosis, rheumatoid arthritis, and obesity5. Physical activity maximizes bone mass, increases bone resistance, and decreases fracture risk35,36. Exercise affects bone remodulation and improves mineralization and geometry35. However, information and a gold standard for the beneficial effects of physical straining on the modulation of inflammatory responses are lacking37.
The findings of this study are promising owing to increased interest in research on the effects of physical activity as a modulator of systemic conditions caused by many inflammatory diseases. Our findings are relevant to the field of sports dentistry, highlighting the need for more studies and the publication of consistent literature on the issue. This study had some limitations. Our results should be extrapolated with caution and new studies are required to better understand the mechanisms and relationships between physical training and AP. Our study revealed the protective effect of physical training during disease progression. Notably, the effects of the chronological occurrence of events could be an important future assessment. New studies could reveal the behavior of AP in individuals with a previous history of physical training and evaluate the local and systemic effects of physical training in individuals after the development of AP.
Conclusion
Physical activity can reduce the damage caused by AP, thereby modifying systemic levels of TNF-α and IL-6, and leading to the minimization of local damages. The changes in the periapical bone based on micro-CT and histological analyses reflected a decrease in bone damage. Therefore, these results support the positive benefits of physical training on inflammatory processes, such as those reported in our AP model. However, further research is needed to elucidate the underlying molecular pathways and evaluate the relevant tissues.
Methods
Ethical aspects and formation of the experimental groups
This study was approved by the Ethics Committee on Experimental Animals of the Federal University of Pará (license number: 4090250320) in accordance with the Guide for the Care and Use of Laboratory Animals and Animal Research: Reporting of In Vivo Experiments (ARRIVE)38. The sample size was calculated using GPower 3.1.9.4 software based on a previous study39.
Thirty-two male Rattus norvegicus Wistar rats (age, 90 days old; weight, ~ 150 g) were obtained from the central vivarium of the Federal University of Pará. The animals were distributed in plastic cages (4 animals each), administered controlled food (Nuvital Nutrientes S/A, Paraná, Brazil) and filtered water ad libitum, and stored in a room under a 12-h light/dark cycle and controlled temperature (25 ± 1 °C).
The animals were divided into four experimental groups (8/per group): control (sedentary animals), AP, physical training (PT), and AP plus physical training (AP + PT). The experimental design is illustrated in Fig. 5.

Description of the methodology. (1) Sample and experimental group descriptions. (2) Induction of apical periodontitis. (3) Physical training protocol. (4) Collection of the biological samples. (5) Measurement of cytokine levels using enzyme-linked immunoassay. (6) Histological evaluation. (7) Assessment of alveolar bone effects using computed microtomography.
Apical periodontitis induction
One day before the beginning of the physical training protocol, animals in the AP and AP + PT groups were anesthetized with intraperitoneal injections of 9 mg/kg 2% xylazine hydrochloride (2 mg/mL) and 90 mg/kg 10% ketamine hydrochloride (10 mg/mL). After anesthesia, the pulp chamber was accessed in the distal fossa of the mandibular first molars using a #1/4 low-speed carbide bur. The pulp chamber was left open for 28 days to enable development of the AP lesions. This method is widely used and accepted according to the literature. Periapical lesions can be established within the required timeframe using this technique9. A daily dosage of buprenorphine (0.05 mg/kg on the day of the procedure and 0.1 mg/kg for the following 2 days). This medication was administered to alleviate pain and discomfort associated with the surgical procedure, including pulp exposure.
Physical training
A motorized treadmill designed for rodents (50 cm long and 10 cm wide) with lanes divided into acrylic walls was employed for the physical training program. The running sessions lasted 30 min each training session. Five sessions were held each week (one session per day) for four consecutive weeks.
This protocol, which comprises exercise intensity (60% VO2 max), was based on the parameters used in previous studies39,40. Each training session began with a 10-min warm-up at a slower speed, followed by a weekly speed schedule. Each week, the distance and running speed were gradually increased (Fig. 1).
Perfusion and sample collection
Animals were anesthetized as previously described. Blood was collected and centrifuged at 3.000 rpm, and the obtained serum was collected and stored in an ultrafreezer at −80 °C for further analysis. The animals were perfused through the left ventricle of the heart with 0.9% saline solution, followed by 4% formaldehyde. The hemimandibles were collected and stored in 4% formaldehyde solution. The left hemimandibles were used for microtomographic analysis, whereas the right hemimandibles were used for histological analysis.
Evaluation of the serum cytokine concentrations
Serum samples (n = 8/group) were analyzed as described previously42. Briefly, the levels of interleukin-1beta (IL-1β) (detection range: 62.5–4000 pg/mL; minimum detection limit: 12.5 ng/mL), interleukin-6 (IL-6) (detection range: 125–8000 pg/mL), interleukin-10 (IL-10) (detection range: 62.5–4000 pg/mL; minimum detection limit: 12.5 ng/mL), and tumor necrosis factor-alpha (TNF-α) (detection range: 62.5–4000 pg/mL; minimum detection limit: 50 ng/mL) were determined using commercial enzyme-linked immunosorbent assay kits (R & D Systems, Minneapolis, MN), according to the manufacturer's instructions. The results are expressed as pg/mL.
Histological evaluation
The right hemimandibles were rinsed under running water for 4 h and then demineralized in 10% ethylenediaminetetraacetic acid (EDTA) for 90 days with weekly solution changes. After demineralization, the samples were rinsed under running water for 4 h. The specimens were dehydrated with alcohol, cleared in xylene, and embedded in paraffin. Sections of 5 μm thickness were cut using a Leica RM 2045 microtome (Leica Microsystems, Nussloch, Germany) in the mesiodistal orientation and mounted on individual slides. The sections were stained with hematoxylin and eosin, and photomicrographed using a digital camera (DS-Fi3; Nikon, Tokyo, Japan) attached to a microscope (Nikon Eclipse CiH550s; Tokyo, Japan). Images were subjected to histopathological analyses.
Bone analysis using computerized microtomography (Micro-CT)
The left hemimandibles were scanned using X-ray micro-CT (MicroCT.SMX-90 CT; Shimadzu Corp., Kyoto, Japan). Images were obtained with a 360° rotation and an intensity of 70 kV and 100 mA. Thereafter, the images were reconstructed using the inspeXio SMX-90CT software (Shimadzu Corp., Kyoto, Japan) with a voxel size of 10 µm, thickness of 14 µm, and resolution of 1024 × 1024, producing 536 photos per sample.
Alveolar bone resorption and alveolar bone tissue quality were analyzed using CTAn software (V1.15.4.0; Bruker, Kontich, Belgium). The alveolar bone resorption area was analyzed as described previously43. The reconstructed volume of interest (VOI) in the sagittal plane was determined, including the periodontal ligament space and destruction around the root of the mandibular first molars. The VOI was determined from the first coronal cut of the mesial root of the mandibular first molar to the last cut in the distal region and ended upon reaching the mandibular second molar.
The quality of the remaining alveolar bone that was unaffected by the lesion was evaluated using a set of approximately 150 images surrounding the roots of the mandibular first molar. The region of interest (ROI) was determined in the transverse plane from the point closest to the mesial root to the point farthest from the distal root. Segmentation was performed on the images with grayscale thresholds ranging from 120 to 225. The following parameters were measured: trabecular thickness (Tb.Th), trabecular spacing (Tb.Sp), trabecular number (Tb.N), and bone volume percentage (BV/TV).
Statistical analyses
Statistical analyses were performed using GraphPad Prism 7.0 software (GraphPad Software Inc., La Jolla, CA, USA). The Shapiro–Wilk test was conducted to assess normality. For comparisons between groups, one-way ANOVA followed by Tukey’s post-hoc test was performed. A p value < 0.05 was considered to indicate statistical significance. The results are presented as mean ± standard error of the mean (SEM). All the values of our analysis are available on the Supplementary Table S1.
Data availability
All the data analyzed in this study is included in this article and in the supplementary table S1.
References
Garber, C. E. et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 43, 1334–1359. https://doi.org/10.1249/MSS.0b013e318213fefb (2011).
Hortobágyi, T. et al. Effects of exercise training on muscle quality in older individuals: A systematic scoping review with meta-analyses. Sports Med. Open 9, 41. https://doi.org/10.1186/s40798-023-00585-5 (2023).
Eckstrom, E., Neukam, S., Kalin, L. & Wright, J. Physical activity and healthy aging. Clin. Geriatr. Med. 36, 671–683. https://doi.org/10.1016/j.cger.2020.06.009 (2020).
Ávila-Gandía, V. et al. High versus low-moderate intensity exercise training program as an adjunct to antihypertensive medication: A pilot clinical study. J. Pers. Med. 11, 291. https://doi.org/10.3390/jpm11040291 (2021).
Hajizadeh Maleki, B. et al. Low-to-moderate intensity aerobic exercise training modulates irritable bowel syndrome through antioxidative and inflammatory mechanisms in women: Results of a randomized controlled trial. Cytokine 102, 18–25. https://doi.org/10.1016/j.cyto.2017.12.016 (2018).
Pedersen, B. K. Exercise-induced myokines and their role in chronic diseases. Brain Behav. Immun. 25, 811–816. https://doi.org/10.1016/j.bbi.2011.02.010 (2011).
Palmefors, H., DuttaRoy, S., Rundqvist, B. & Börjesson, M. The effect of physical activity or exercise on key biomarkers in atherosclerosis: A systematic review. Atherosclerosis 235, 150–161. https://doi.org/10.1016/j.atherosclerosis.2014.04.026 (2014).
Braz-Silva, P. H. et al. Inflammatory profile of chronic apical periodontitis: A literature review. Acta Odontol. Scand. 77, 173–180. https://doi.org/10.1080/00016357.2018.1521005 (2019).
Goldman, E. et al. A mouse model for studying the development of apical periodontitis with age. Cells 10, 671. https://doi.org/10.3390/cells10030671 (2021).
Kalatzis-Sousa, N. G., Spin-Neto, R., Wenzel, A., Tanomaru-Filho, M. & Faria, G. Use of micro-computed tomography for the assessment of periapical lesions in small rodents: A systematic review. Int. Endod. J. 50, 352–366. https://doi.org/10.1111/iej.12633 (2017).
Gomes, M. S. et al. Can apical periodontitis modify systemic levels of inflammatory markers? A systematic review and meta-analysis. J. Endod. 39, 1205–1217. https://doi.org/10.1016/j.joen.2013.06.014 (2013).
Lang, N. P. & Bartold, P. M. Periodontal health. J. Clin. Periodontol. 45, S9–S16. https://doi.org/10.1111/jcpe.12936 (2018).
Sehirli, A. et al. Protective effect of alpha-lipoic acid against apical periodontitis-induced cardiac injury in rats. Eur. J. Oral Sci. 127, 333–339. https://doi.org/10.1111/eos.12618 (2019).
Aksoy, U. et al. Effects of alpha-lipoic acid therapy on experimentally induced apical periodontitis: A biochemical, histopathological and micro-CT analysis. Int. Endod. J. 52, 1317–1326. https://doi.org/10.1111/iej.13121 (2019).
Tibúrcio-Machado, C. S. et al. The global prevalence of apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 54, 712–735. https://doi.org/10.1111/iej.13467 (2021).
Palma, P. J. et al. Histologic evaluation of regenerative endodontic procedures with the use of chitosan scaffolds in immature dog teeth with apical periodontitis. J. Endod. 43, 1279–1287. https://doi.org/10.1016/j.joen.2017.03.005 (2017).
Yamauchi, N. et al. Tissue engineering strategies for immature teeth with apical periodontitis. J. Endod. 37, 390–397. https://doi.org/10.1016/j.joen.2010.11.010 (2011).
Verma, P. et al. Effect of residual bacteria on the outcome of pulp regeneration in vivo. J. Dent. Res. 96, 100–106. https://doi.org/10.1177/0022034516671499 (2017).
Cosme-Silva, L. et al. Reduced bone resorption and inflammation in apical periodontitis evoked by dietary supplementation with probiotics in rats. Int. Endod. J. 53, 1084–1092. https://doi.org/10.1111/iej.13311 (2020).
Park, O. J. et al. A pilot study of chronological microbiota changes in a rat apical periodontitis model. Microorganisms 8, 1174. https://doi.org/10.3390/microorganisms8081174 (2020).
Poornima, L., Ravishankar, P., Abbott, P. V., Subbiya, A. & PradeepKumar, A. R. Impact of root canal treatment on high-sensitivity C-reactive protein levels in systemically healthy adults with apical periodontitis: A preliminary prospective, longitudinal interventional study. Int. Endod. J. 54, 501–508. https://doi.org/10.1111/iej.13444 (2021).
Jang, D. I. et al. The role of tumor necrosis factor alpha (TNF-α) in autoimmune disease and current TNF-α inhibitors in therapeutics. Int. J. Mol. Sci. 22, 2719. https://doi.org/10.3390/ijms22052719 (2021).
Wang, L. et al. The potential roles of t cells in periapical lesions. J. Endod. 48, 70–79. https://doi.org/10.1016/j.joen.2021.09.016 (2022).
Wang, B. et al. Metabolism pathways of arachidonic acids: Mechanisms and potential therapeutic targets. Signal Transd. Target. Therapy 6, 94. https://doi.org/10.1038/s41392-020-00443-w (2021).
Minhoto, G. B., Khoury, R. D., Orozco, E. I. F., Prado, R. F. & Valera, M. C. Effect of chronic unpredictable stress on the progression of experimental apical periodontitis in rats. Int. Endod. J. 54, 1342–1352. https://doi.org/10.1111/iej.13515 (2021).
Zhou, S. et al. The specific morphological features of alveolar bone. J. Craniofac. Surg. 29, 1216–1219. https://doi.org/10.1097/scs.0000000000004395 (2018).
Chen, S. et al. Effects of chronic apical periodontitis on the inflammatory response of the aorta in hyperlipemic rats. Clin. Oral Investig. 25, 3845–3852. https://doi.org/10.1007/s00784-020-03714-6 (2021).
Cotti, E. et al. Healing of apical periodontitis in patients with inflammatory bowel diseases and under anti–tumor necrosis factor alpha therapy. J. Endod. 44, 1777–1782. https://doi.org/10.1016/j.joen.2018.09.004 (2018).
Azuma, M. M. et al. Omega 3 fatty acids reduce bone resorption while promoting bone generation in rat apical periodontitis. J. Endod. 43, 970–976. https://doi.org/10.1016/j.joen.2017.01.006 (2017).
Martinho, F. C. et al. Clinical influence of different intracanal medications on Th1-type and Th2-type cytokine responses in apical periodontitis. J. Endod. 41, 169–175. https://doi.org/10.1016/j.joen.2014.09.028 (2015).
Lukić, A. et al. Characterization of antigen-presenting cells in human apical periodontitis lesions by flow cytometry and immunocytochemistry. Int. Endod. J. 39, 626–636. https://doi.org/10.1111/j.1365-2591.2006.01125.x (2006).
Andrade, E. F. et al. Physical exercise improves glycemic and inflammatory profile and attenuates progression of periodontitis in diabetic rats (HFD/STZ). Nutrients 10, 1702. https://doi.org/10.3390/nu10111702 (2018).
Wei, L., Xu, M. & Xiong, H. J. O. D. An update of knowledge on the regulatory role of Treg cells in apical periodontitis. Oral Dis. 27, 1356–1365. https://doi.org/10.1111/odi.13450 (2021).
Ferreira, R. D. O. et al. Physical activity reduces the prevalence of periodontal disease: Systematic review and meta-analysis. Front. Physiol. 10, 437689. https://doi.org/10.3389/fphys.2019.00234 (2019).
Babatunde, O. O., Bourton, A. L., Hind, K., Paskins, Z. & Forsyth, J. J. Exercise interventions for preventing and treating low bone mass in the forearm: A systematic review and meta-analysis. Archiv. Phys. Med. Rehabil. 101, 487–511. https://doi.org/10.1016/j.apmr.2019.07.007 (2020).
Weaver, C. M. et al. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos. Int. 27, 1281–1386. https://doi.org/10.1007/s00198-015-3440-3 (2016).
Cerqueira, É., Marinho, D. A., Neiva, H. P. & Lourenço, O. Inflammatory effects of high and moderate intensity exercise—A systematic review. Front. Physiol. 10, 1550. https://doi.org/10.3389/fphys.2019.01550 (2020).
Percie du Sert, N. et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 18, e3000410. https://doi.org/10.1371/journal.pbio.3000410 (2020).
Pamplona-Santos, D. et al. Aerobic physical exercise as a neuroprotector strategy for ethanol binge-drinking effects in the hippocampus and systemic redox status in rats. Oxid. Med. Cell Longev. https://doi.org/10.1155/2019/2415243 (2019).
Arida, R. M. et al. Physical training in developing rats does not influence the kindling development in the adult life. Physiol. Behav. 90, 629–633. https://doi.org/10.1016/j.physbeh.2006.11.016 (2007).
Peinado, B. R. R. et al. Physical exercise mitigates salivary gland and saliva damages in rats exposed to binge-like ethanol pattern. Antioxidants 12, 1038. https://doi.org/10.3390/antiox12051038 (2023).
Safieh-Garabedian, B., Poole, S., Allchorne, A., Winter, J. & Woolf, C. J. Contribution of interleukin-1 beta to the inflammation-induced increase in nerve growth factor levels and inflammatory hyperalgesia. Br. J. Pharmacol. 115, 1265–1275. https://doi.org/10.1111/j.1476-5381.1995.tb15035.x (1995).
Chen, S. et al. Micro-CT analysis of chronic apical periodontitis induced by several specific pathogens. Int. Endod. J. 52, 1028–1039. https://doi.org/10.1111/iej.13095 (2019).
Acknowledgements
We thank Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento Pessoal de Ensino Superior (CAPES), Fundação de Amparo e Desenvolvimento da Pesquisa (FADESP), and Pró-reitoria de Pesquisa da Universidade Federal do Pará (PROPESP-UFPA) for the fellowships provided for this study.
Funding
R.R.L. is a researcher at Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and received a grant (312275/2021-8). This research was also funded by PROCAD Amazônia CAPES (23038.005350/2018-78). The APC was funded by the Pró-Reitoria de Pesquisa e Pós-graduação of the Federal University of Pará (PROPESP-UFPA).
Author information
Authors and Affiliations
Contributions
Conceptualization: M.S.P., R.O.F., R.R.L.; Methodology: D.S-M, D.R.F., J.D.M.M, M.L.S.L, and A.A.A.; Formal analysis: LO.B., D.C.B.S., A.A.A, and R.R.L.; Resources: G.S.B and F.M.C.; Data curation: R.O.F., L.O.B., and R.R.L.; Writing Original draft preparation: M.S.P, D.S-M, D.C.B.S., R.O.F., and L.O.B.; Writing, review and editing: D.S-M, D.R.F., J.D.M.M., L.O.B., and R.R.L.; Visualization: G.S.B, F.M.C., A.A.A, and R.R.L.; Supervision: R.R.L.; Project administration: R.R.L.; and Funding acquisition: R.R.L. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ferreira, R.d., Pereira, M.S., Souza-Monteiro, D. et al. Physical training attenuates systemic cytokine response and tissue damage triggered by apical periodontitis. Sci Rep 14, 8030 (2024). https://doi.org/10.1038/s41598-024-58384-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-58384-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
